Mental health disparities are significant
concern in many countries, including India.
There are various factors that contribute to
disparities in mental health services
utilisation, including socio-economic status,
caste, gender, and cultural beliefs. These disparities can lead to inadequate access to
mental health services and can result in
negative outcomes for individuals and
communities.
Caste is a significant factor that has been
shown to play a role in mental health
disparities in India. The caste system, which
is deeply ingrained in Indian society, has
resulted in significant social and economic
disparities between castes, leading to unequal
access to education, employment, and
healthcare, including mental health services.
Individuals from lower castes are less likely
to seek mental health services and are more
likely to receive inadequate care when they
do seek help. There are various reasons for
this, including lack of awareness and
education about mental health, stigma
associated with mental illness, cultural and
religious beliefs, and financial constraints.
Mental health policies can also prioritise a
preventive approach. To the extent that
discrimination and violence contribute to
depression and anxiety in India, reducing
them would improve overall mental health.
This is especially relevant in low-resource
settings such as India, where access to mental
healthcare is extremely limited.
Women also face various social and cultural
barriers that limit their access to mental
health services. To address these disparities,
it is essential to increase awareness and
education about mental health, reduce the
stigma associated with mental illness, and
provide accessible and affordable mental
health services to all individuals, regardless
of their caste, gender, or socioeconomic
status. This can be achieved through various
means, such as community-based mental
health programs, tele-mental health services,
and initiatives to reduce stigma and
discrimination. In India, there is significant
mental health treatment gap, with only a small
percentage of individuals seeking and
receiving appropriate care. This treatment
gap is even more pronounced for marginalised
populations, such as those belonging to lower
castes and women. Women and individuals
from lower castes are less likely to utilise
mental health services than men and those
from higher castes. Women are more likely
to report mental health problems than men,
but they are less likely to seek help. To
address these disparities, there is a need for
culturally sensitive and accessible mental
health services that are tailored to the specific
needs of different social groups. This may
involve increasing awareness about mental
health issues, reducing stigma, and providing
affordable and accessible mental health
services in both urban and rural areas. Efforts
should be made to empower women and
individuals from lower castes to seek and
receive mental health services by addressing
the underlying social and economic factors
that contribute to these disparities.
The study’s conclusions are consistent with
earlier investigations in same circumstances.
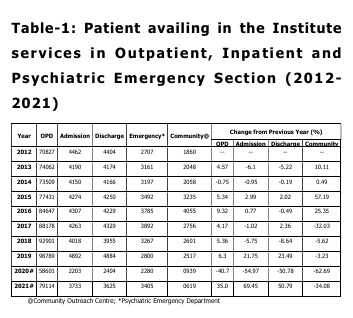
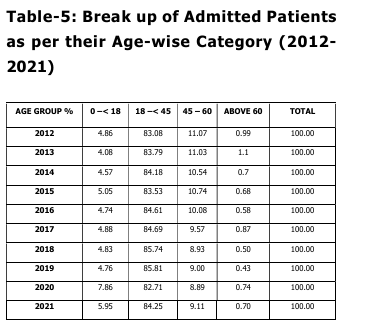
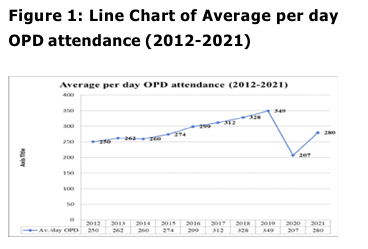
According to Table 1 of the current study,
there was a more than 28% rise in patient
registration at the OPD level in just ten years.
Several factors or variables may be
responsible for it, such as the “marked
increase in the global burden of disease
sharing mental, neurological, and substance
use” (WHO, 2004; Haldar et al., 2017), the
“notoriety for the rise in mental, neurological,
and substance use disorders” (Patel et al.,
2016), the “limited availability and
accessibility of basic and specialised mental
health services at primary and secondary
levels in this region of the country,” the
“growing awareness about mental illness,” etc.
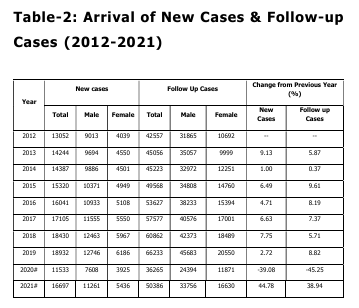
Notedly, men have consistently made up the
vast majority of females in both new and
follow-up cases (Table 2). Table 2 shows that,
when it came to new cases, or patients who
were visiting the Institute for the first time,
the proportion of male patients nearly doubled
between 2012 and 2021 and increased to over
2.5 times at the follow-up.
This implies that women receive fewer
tertiary-level treatments for mental diseases
than men do, and that women patients also
attend fewer routine follow-up appointments.
Studies on the use of mental health services
in metropolitan India have revealed a ratio of
one woman to every three men visiting public
health psychiatric outpatient clinics. This
suggests that afflicted women “under-utilize”
available resources. There is a likely greater
stigma attached to women’s mental illness that
negatively impacts the help-seeking behaviour
for public mental health facilities, and/or
lesser importance is given to mental health
issues pertaining to women in general.
The reasons for this gender gap in treatment
seeking and follow-up are multifaceted and
include both sociocultural and illness-related
factors. These include the following: “possible
impact of gender on the age of onset of
symptoms, clinical features, frequency of
psychotic symptoms, course, social
adjustment, and long-term outcome of severe
mental disorders”; “forms of social support
available and accessible to women with mental
illnesses”; and, most importantly, “anticipating
societal rejection in the forms of stigma,
stereotypes, and prejudices for mentally ill
women and their carers” (Malhotra & Shah,
2015).
The difference between prevalence and use
can increase with gender. One possible
explanation for this low attendance rate is the
dearth of resources designed specifically to satisfy the requirements of women in hospital
settings. The sex-based disparity in bed
availability indicates that most mental
hospitals appear to favourably assign health
facilities to men. In government mental health
facilities, the male-to-female bed ratio is
73%:27%, whereas the ratio for individuals
involved in service, research, and training is
66%:34% (Davar, 1999; Sood, 2008; Malhotra
& Shah, 2015).
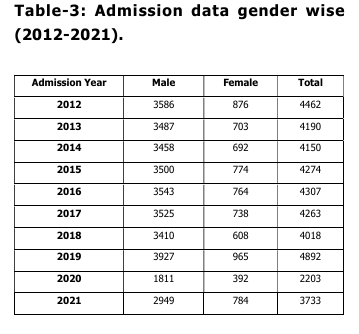
The predominance of males in the utilisation
of services, which is observed in the present
study, is consistent with previous
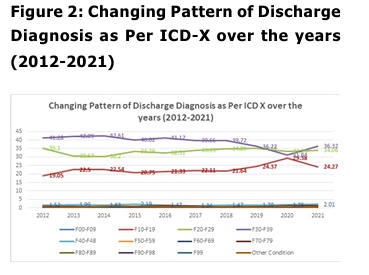
observations. In relation to diagnoses of
discharged patients of the last ten years under
study (2012-2021), a preponderance of mainly
three types of diagnoses was found viz., ‘Mood
[affective]
disorders
(F30-F39)’,
‘ Schizophrenia, schizotypal & delusional
disorders (F20-F29)’ and ‘Mental &
behavioural disorders due to psychoactive
substance use (F10-F19)’, with ‘Mood
Disorders’ being the most common diagnosis,
followed by Schizophrenia, schizotypal &
delusional disorders’ and ‘Mental &
behavioural disorders due to psychoactive
substance use’ (Figure-2).
Institute being a tertiary or referral one;
hence, people with severe mental disorders
like the three mentioned above tend to come
here to receive intensive treatment. Another
possible reason could be that people with
other psychiatric diagnoses do not opt for
admission into the current study’s assessment
of a male preponderance in service use is in
line with earlier findings. The diagnoses of
patients who were discharged during the last
ten years under study (2012–2021) mostly fell
into three categories: “Mood [affective]
disorders (F30–F39),” “Schizophrenia,
schizotypal & delusional disorders (F20–F29),”
and “Mental & behavioural disorders due to
psychoactive substance use (F10–F19).” The
most common diagnosis was “Mood
Disorders,” which was followed by
“Schizophrenia, schizotypal & delusional
disorders” and “Mental & behavioural
disorders due to psychoactive substance use”
(Figure-2). Inpatient wards and would much
rather receive care in an outpatient
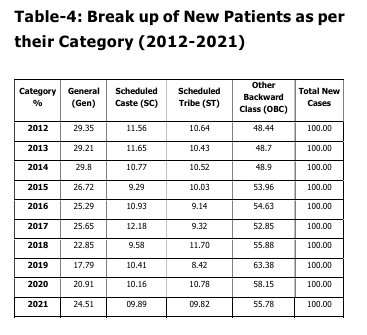
department. An essentially identical pattern
was seen with regard to the age and category
of patients admitted throughout the last 10
years (2012–2021), with a preponderance of
individuals falling into the 18–45 age groups
and the Other Backwards Classes (OBC)
category.
According to several previous epidemiological
studies (Verghese et al., 1985; Fenton &
McGlashan, 1991; Thara, Padmavati &
Nagaswami, 1993; Wig et al., 1993; Kulhara,
Shah & Aarya, 2010; Rao, 2010; Baxter et al.,
2016; Murthy, 2017), the preponderance of
age group can be attributed to a higher
prevalence and incidence of severe and
common mental disorders in this age group.
According to a National Sample Survey
Organisation (NSSO) survey, 40.94% of the
population is OBC, 19.59% is SC, and 8.63%
is ST. The other 30.80% of people make up
the remaining population. Therefore, the
population’s demographics can explain the
preponderance of persons belonging to the
OBC Category in the discharged list.
Baxter, A.J., Charlson, F.J., Cheng, H.G.,
Shidhaye, R., Ferrari, A.J., &
Whiteford, H.A. (2016). Prevalence of
mental, neurological, and substance
use disorders in China and India: A
systematic analysis. The Lancet
Psychiatry, 3(9), 832 – 841. http://
d x.doi.org/10.1016/S2215
0366(16)30139-0
Charlson, F.J., Baxter, A.J., Cheng, H.G.,
Shidhaye, R., & Whiteford, H.A.
(2016). The burden of mental,
neurological, and substance use
disorders in China and India: A systematic analysis of community
representative epidemiological
studies. The Lancet, 388(10042), 376
389.
Davar, B.V. (1999). Mental Health of Indian
Women – A Feminist Agenda. New
Delhi/Thousand Oaks/London: Sage
Publications.
Fenton, W.S., & McGlashan, T.H. (1991).
Natural History of Schizophrenia
Subtypes-II. Positive and Negative
Symptoms and Long-term Course.
Archives of General Psychiatry, 48(11),
978–986.
doi:10.1001/
archpsyc.1991.01810350018003
Haldar, P., Sagar, R., Malhotra, S., & Kant, S.
(2017). Burden of psychiatric
morbidity among attendees of a
secondary level hospital in Northern
India: Implications for integration of
mental health care at subdistrict level.
Indian Journal of Psychiatry, 59(2),
176-182.
doi:
[10.4103/
psychiatry.IndianJPsychiatry_324_16]
Kulhara, P., Shah, R., & Aarya, K.R. (2010).
An overview of Indian research in
schizophrenia. Indian Journal of
Psychiatry, 52(Suppl 1), S159-S172.
doi: [10.4103/0019-5545.69229]
Lakhan, R., & Ekúndayò, O.T. (2015). National
sample survey organization survey
report: An estimation of prevalence of
mental illness and its association with
age in India. Journal of Neuroscience
in Rural Practice, 6(1), 51-54. doi:
10.4103/0976-3147.143194.
Malhotra, S., & Shah, R. (2015). Women and
mental health in India: An overview.
Indian Journal of Psychiatry, 57(Suppl
2), S205-S211. doi: [10.4103/0019
5545.161479]
Math, S.B., & Srinivasaraju, R. (2010). Indian
Psychiatric epidemiological studies:
Learning from the past. Indian Journal
of Psychiatry, 52(Suppl 1), S95-S103.
Murthy, R.S. (2017). National mental health
survey of India 2015–2016. Indian
Journal of Psychiatry, 59, 21-26
Nizamie, S.H., Goyal, N., Haq, M.Z., & Akhtar,
S. (2008). Central Institute of
Psychiatry: A tradition in excellence.
Indian Journal of Psychiatry, 50(2),
144-148. doi: 10.4103/0019
5545.42405
Patel, V., & Thornicroft, G. (2009). Packages
of care for mental, neurological, and
substance use disorders in low-and
middle-income countries: PLoS
Medicine Series. PLoS medicine,
6(10), e1000160. doi: https://doi.org/
10.1186/1752-4458-8-30
Patel, V., Chisholm, D., Parikh, R., Charlson,
F.J., Degenhardt, L., Dua, T., Ferrari,
A.J., Hyman, S., Laxminarayan, R.,
Levin, C., Lund, C., Medina Mora, M.E.,
Petersen, I., Scott, J., Shidhaye, R.,
Vijayakumar, L., Thornicroft, G., &
Whiteford, H., DCP MNS Author Group
(2016). Addressing the burden of
mental, neurological, and substance
use disorders: Key messages from
Disease Control Priorities, 3rd edition.
The Lancet, 387(10028), 1672-1685.
Rao, P.G. (2010). An overview of Indian
research in bipolar mood disorder.
Indian Journal of Psychiatry, 52(Suppl
1), S173-S177. doi: [10.4103/0019
5545.69230]
Report of the Working Group on Tertiary Care
Institutions for 12th Five Year Plan
(2012-2017). No. 2 (6)2010-H&FW,
Government of India, Planning
Commission. Downloaded from: http:/
/planningcommission.nic.in/aboutus/
c ommittee/wrkgrp12/health/
WG_2tertiary.pdf
Sood, A. (2008). Women’s Pathways to Mental
Health in India. UC Los Angeles: UCLA
Center for the Study of Women. 2008.
Downloaded
f rom:
http://www.escholarship.org/uc/item/
0nd580×9.
Thara, R., Padmavati, R. & Nagaswami, V.
(1993). Schizophrenia in India.
Epidemiology, Phenomenology, Course
and Outcome, International Review of
Psychiatry, 5(2-3), 157-164, DOI:
10.3109/09540269309028306
Verghese, A., Dube, K.C., John, J., Menon,
D.K., Menon, M.S., Rajkumar, S.,
Richard, J., Sethi, B.B., Trivedi, J.K.,
& Wig, N.N. (1985). Factors
associated with the course and
outcome of schizophrenia. Indian
Journal of Psychiatry, 27(3), 201-206.
Wasylenki, D., Goering, P., Cochrane, J.,
Durbin, J., Rogers, J., & Prendergast,
P. (2000). Tertiary mental health
services: I. Key concepts. Canadian
Journal Psychiatry, 45(2), 179-184.
doi:
https://doi.org/10.1177/
070674370004500209
Wig, N.N., Varma, V.K., Mattoo, S.K., Behere,
P.B., Phookan, H.R., Misra, A.K.,
Murthy, R.S., Tripathi, B.M., Menon,
D.K., Khandelawal, S.K., & Bedi, H.
(1993). An incidence study of
schizophrenia in India. Indian Journal
of Psychiatry, 35(1), 11-17.
World Health Organization (2004). The Global
Burden of Disease: 2004 Update.
Geneva, Switzerland: WHO Press.
World Health Organization (2008). mhGAP:
Mental Health Gap Action Programme:
Scaling up care for mental,
neurological and substance use
disorders.
Zachariah, A. (2012). Tertiary Healthcare
within a Universal System: Some
Reflections. Economic & Political
Weekly, Vol XLVII (12), 39-45.