
Indian Journal of Health Social Work
(UGC CARE List Journal)
EMOTION REGULATION AND INSOMNIA AMONG CAREGIVERS
OF PERSONS WITH ALCOHOL USE DISORDER
Lokesh Kumar Ranjan1 & Deena Nath Yadav2
1PhD Scholar, 2Assitant Professor & Head, Department of Social Work, MATS
University, Raipur, Chhattisgarh, India
Correspondence: Lokesh Kumar Ranjan, e-mail: lokeshr00@gmail.com
ABSTRACT
Background: Alcohol use disorder (AUD) affects families globally. Providing care for individuals
with AUD can disrupt emotional regulation and contribute to insomnia among family members.
Chhattisgarh state has higher prevalence of alcohol use India. It is important to examine how the
behavior of individuals with AUD impacts the emotion regulation and sleep of caregivers.
Aim: To assess and compare emotional regulation and insomnia among caregivers of persons
with alcohol use disorder in relapse and remission. Methods: Present study used descriptive
cross-sectional comparative research design. Study was conducted at IPD & OPD of CIIMHANS,
Dewada, Chhattisgarh, India. A total of 200 sample (100 caregivers of persons with AUD in
relapse and 100 caregivers of persons with AUD in remission) were selected from purposive
sampling. Socio-demographic and clinical datasheet, The Emotional Regulation Scale and Insomnia
Severity Index (ISI) were used. Results: Caregivers of persons with AUD in relapse group reported
greater difficulties in emotional regulation and sleep disturbances compared to caregivers of
persons with AUD in remission. Emotion regulation showed significant positive correlation with
insomnia and in regression analysis further indicated that emotion regulation accounted for about
89.7% of the variance in insomnia among caregivers. Conclusion: Caregiving for persons with
AUD, particularly during relapse, is linked to greater difficulties in emotional regulation and
significant sleep disturbances. These findings highlight the need for holistic, family-focused
interventions that address both emotion regulation and sleep difficulties to improve treatment
outcomes for persons with AUD and enhance caregiver wellbeing.
Keywords: alcohol use disorder, emotion regulation, insomnia, caregiver.
Submitted: 03.09.2025 Revised: 09.10.2025 Accepted: 01.11.2025 Published: 28.01.2026
How to cite this article: Ranjan, L. K., & Yadav, D. N. (2025). Emotion regulation and insomnia
among caregivers of persons with alcohol use disorder. Indian Journal of Health Social Work,
7(2), 53-60.
INTRODUCTION
Alcohol Use Disorder (AUD) represents the
advanced stage of alcohol addiction, marked
by tolerance, where increasing amounts of
alcohol are needed to achieve the same effect (Edwards & Gross, 1986). The World Health
Organization reported that harmful alcohol
use was responsible for 3 million deaths (5.3%
of all deaths) and 132.6 million disability
adjusted life years (DALYs, 5.1%) in 2016
(Glantz et al., 2020; Lui et al., 2023). In India,
the National Health Survey (2016) estimated
17% (10.6 million) of the population were
alcohol dependent (Gautham et al., 2020),
with Chhattisgarh reporting the highest
prevalence at 35.6% (Ambekar et al., 2019).
Globally, AUD continues to be a major public
health concern, with relapse rates ranging
between 40% and 60% even after treatment
(Moos & Moos, 2006). The recurrent nature
of relapse not only affects persons with AUD
but also places significant psychological,
emotional, and physical strain on their
caregivers (Kalra & Tung, 2024).
A caregiver, or “carer,” is someone who
provides support to a person whose
functioning is limited by illness, disability, or
age. Caregiving responsibilities may include
assisting with daily activities, managing
medical needs, providing emotional support,
and ensuring overall well-being (Ortelli,
2021). In the context of AUD, caregivers often
report emotional exhaustion, irritability, and
helplessness, reflecting difficulties in
managing their own emotions (Sharma et al.,
2021).
Emotion regulation, defined as the ability to
monitor, evaluate, and modify emotional
responses in adaptive ways (Gross, 2015), is
especially important for caregivers. Those
caring for persons with AUD frequently face
heightened stress, disrupted routines, and
emotional challenges, compounded by the
social stigma associated with addiction
(Orford et al., 2010). Poor emotion regulation
among caregivers has been linked to greater
psychological distress, interpersonal conflicts,
and reduced resilience (Cousino & Hazen,
2013). Relapse episodes further complicate
caregiving, as the unpredictability of the
patient’s behavior intensifies emotional strain.
Insomnia, defined as persistent difficulties
with sleep initiation, maintenance, or quality,
is strongly associated with caregiving burden
(McCurry et al., 2007). Emotional instability
and psychological distress are often
influenced by chronic sleep disturbances and
vice versa (Palmer & Alfano, 2017).
Research has pointed out that elevated
stress, disturbed sleep, and weakened
immunity, makes cager giver more vulnerable
to health problems (Sen et al., 2016).
Moreover, the duration of caregiving has been
correlated with declining sleep pattern, as
longer caregiving periods increase the risk of
chronic conditions (Kumar Goit et al., 2021).
Despite the significant burden faced by
caregivers, relatively few studies have
examined their experiences, particularly in the
Indian context. Exploring how emotion
regulation and insomnia differ among
caregivers of persons with AUD in relapse
versus remission is essential to understanding
their unique stressors and protective factors,
and to inform strategies that can promote
caregiver well-being.
METHODS
Present study used descriptive cross-sectional comparative research design. Study was conducted at IPD & OPD of Central India Institute of Mental Health and Neuro Sciences (CIIMHANS), Dewada, Chhattisgarh, India. The caregivers of persons with alcohol use disorder in relapse and remission were selected using purposive sampling. A total of 200 caregivers (100 caregivers of persons with AUD in relapse and 100 caregivers of persons with AUD in remission) were selected for assessment and comparison of emotional regulation and insomnia. The caregivers were described about the study and those gave written informed consent were selected for further assessment. Socio-demographic and clinical datasheet, The Emotional Regulation Scale and Insomnia Severity Index (ISI) were used. Study was approved from the Ethics Committee of CIIMAHNS.
Present study used descriptive cross-sectional comparative research design. Study was conducted at IPD & OPD of Central India Institute of Mental Health and Neuro Sciences (CIIMHANS), Dewada, Chhattisgarh, India. The caregivers of persons with alcohol use disorder in relapse and remission were selected using purposive sampling. A total of 200 caregivers (100 caregivers of persons with AUD in relapse and 100 caregivers of persons with AUD in remission) were selected for assessment and comparison of emotional regulation and insomnia. The caregivers were described about the study and those gave written informed consent were selected for further assessment. Socio-demographic and clinical datasheet, The Emotional Regulation Scale and Insomnia Severity Index (ISI) were used. Study was approved from the Ethics Committee of CIIMAHNS.
Description of tools
Semi-structured of socio-demographic:
The sociodemographic datasheet will be developed for the present study consist of variables such as age, relative of patient, education, occupation, family income, and domicile. The Difficulties in Emotion Regulation Scale 16 (DERS-16), developed by Bjureberg et al. (2016), is a 16-item tool designed to assess problems related to emotion regulation. It evaluates five dimensions: nonacceptance of negative emotions (3 items), difficulty maintaining goals during distress (3 items), problems with impulse control (3 items), limited access to regulation strategies (5 items), and lack of emotional clarity (2 items). Responses are given on a 5-point Likert scale ranging from 1 (almost never) to 5 (almost always). The scale has demonstrated strong i nternal consistency (Cronbach’s alpha between 0.92 and 0.94) and good test–retest reliability (r = 0.85). A total score is calculated by summing all items, with higher scores reflecting greater difficulties, while subscale scores may also be derived. The Insomnia Severity Index (ISI) is a self report questionnaire that measures the perceived severity of insomnia symptoms and their effect on daytime functioning (Bastien et al., 2001). It consists of 5 items rated on a Likert scale, with higher scores indicating more severe insomnia. Total scores are interpreted as follows: 0–7 (no insomnia), 8 14 (subthreshold insomnia), 15–21 (moderate insomnia), and 22–28 (severe insomnia). The ISI has shown adequate reliability, with Cronbach’s alpha ranging from 0.74 to 0.91 and test–retest reliability at 0.84.
Semi-structured of socio-demographic:
The sociodemographic datasheet will be developed for the present study consist of variables such as age, relative of patient, education, occupation, family income, and domicile. The Difficulties in Emotion Regulation Scale 16 (DERS-16), developed by Bjureberg et al. (2016), is a 16-item tool designed to assess problems related to emotion regulation. It evaluates five dimensions: nonacceptance of negative emotions (3 items), difficulty maintaining goals during distress (3 items), problems with impulse control (3 items), limited access to regulation strategies (5 items), and lack of emotional clarity (2 items). Responses are given on a 5-point Likert scale ranging from 1 (almost never) to 5 (almost always). The scale has demonstrated strong i nternal consistency (Cronbach’s alpha between 0.92 and 0.94) and good test–retest reliability (r = 0.85). A total score is calculated by summing all items, with higher scores reflecting greater difficulties, while subscale scores may also be derived. The Insomnia Severity Index (ISI) is a self report questionnaire that measures the perceived severity of insomnia symptoms and their effect on daytime functioning (Bastien et al., 2001). It consists of 5 items rated on a Likert scale, with higher scores indicating more severe insomnia. Total scores are interpreted as follows: 0–7 (no insomnia), 8 14 (subthreshold insomnia), 15–21 (moderate insomnia), and 22–28 (severe insomnia). The ISI has shown adequate reliability, with Cronbach’s alpha ranging from 0.74 to 0.91 and test–retest reliability at 0.84.
Statistical Analysis
Statistical analyses for the study was conducted using the Statistical Package for the Social Sciences (SPSS) version 25.0. Descriptive demographic variables, such as gender and socioeconomic status, was analyzed using means, standard deviations (SD), and Chi-square tests. To compare the differences between study variables in the two groups (caregivers of persons with AUD and AUD in remission), mean values and standard deviations was calculated, and a t-test was applied to assess significance. Pearson’s correlation was used to examine the relationships between emotional regulation and insomnia among caregivers of persons with alcohol use disorder. A p-value of less than 0.05 was considered statistically significant for all analyses in the study.
Statistical analyses for the study was conducted using the Statistical Package for the Social Sciences (SPSS) version 25.0. Descriptive demographic variables, such as gender and socioeconomic status, was analyzed using means, standard deviations (SD), and Chi-square tests. To compare the differences between study variables in the two groups (caregivers of persons with AUD and AUD in remission), mean values and standard deviations was calculated, and a t-test was applied to assess significance. Pearson’s correlation was used to examine the relationships between emotional regulation and insomnia among caregivers of persons with alcohol use disorder. A p-value of less than 0.05 was considered statistically significant for all analyses in the study.
Ethical Clearance
The present study was conducted after obtaining approval from the Ethics Research Committee of CIIMHANS, Dewada. Written informed consent was obtained from all participants prior to data collection. Participants were assured of the confidentiality and anonymity of their responses, and they were informed that participation was voluntary with the right to withdraw at any stage without penalty.
The present study was conducted after obtaining approval from the Ethics Research Committee of CIIMHANS, Dewada. Written informed consent was obtained from all participants prior to data collection. Participants were assured of the confidentiality and anonymity of their responses, and they were informed that participation was voluntary with the right to withdraw at any stage without penalty.
RESULTS
Table 1 shows the sociodemographic details of caregivers of persons with alcohol use disorder in relapse and remission groups. The mean age of caregivers was similar across groups (46.74 years, SD = 9.27 in relapse and 46.57 years, SD = 11.41 in remission). In terms of relationship, wives constituted the largest group of caregivers (61% in relapse and 51% in remission). In education, the highest proportion of caregivers were graduates in both groups (34%). Most caregivers were employed (78% in relapse and 77% in remission), while rural areas accounted for the largest share of domicile (46% in relapse and 41% in remission). With regard to family income, the majority earned more than ¹ 25,000 per month (45% in relapse and 44% in remission). Overall analysis indicated that there were no statistically significant differences between relapse and remission groups across sociodemographic characteristics including age, relationship, education, occupation, domicile, and family income. India. According to Census 2011 (ORGI, 2011), they comprise 8.6 % of India’s total population, which was 8.2% in the 2001 Census. There are 705 registered distinct tribal groups in India that display uniqueness in socio-cultural and ethnic-lingual arenas,
Table 1 shows the sociodemographic details of caregivers of persons with alcohol use disorder in relapse and remission groups. The mean age of caregivers was similar across groups (46.74 years, SD = 9.27 in relapse and 46.57 years, SD = 11.41 in remission). In terms of relationship, wives constituted the largest group of caregivers (61% in relapse and 51% in remission). In education, the highest proportion of caregivers were graduates in both groups (34%). Most caregivers were employed (78% in relapse and 77% in remission), while rural areas accounted for the largest share of domicile (46% in relapse and 41% in remission). With regard to family income, the majority earned more than ¹ 25,000 per month (45% in relapse and 44% in remission). Overall analysis indicated that there were no statistically significant differences between relapse and remission groups across sociodemographic characteristics including age, relationship, education, occupation, domicile, and family income. India. According to Census 2011 (ORGI, 2011), they comprise 8.6 % of India’s total population, which was 8.2% in the 2001 Census. There are 705 registered distinct tribal groups in India that display uniqueness in socio-cultural and ethnic-lingual arenas,
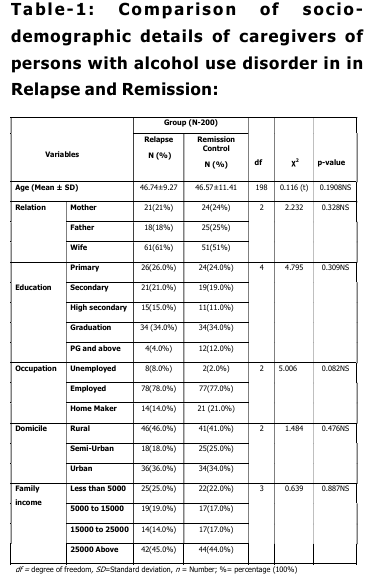
Table 2 shows a comparison of emotional
regulation among caregivers of persons with
alcohol use disorder in relapse and remission
groups. The mean score of non-acceptance
was higher in the relapse group (9.92 ± 3.10)
compared to the remission group (7.69 ±
3.49). The mean score of goal direction was
also higher among caregivers in relapse (8.47
± 0.85) than remission (7.37 ± 3.31). For
impulse control, caregivers in relapse scored
higher (9.90 ± 1.98) than those in remission
(7.70 ± 3.78). Similarly, the mean score of
strategies was greater in relapse (15.13 ±
2.75) compared to remission (9.89 ± 5.03).
The lack of clarity score was also higher in
relapse (4.85 ± 1.59) compared to remission
(3.97 ± 1.92). Overall, the total emotional
regulation score was markedly higher in
relapse (48.27 ± 9.35) than remission (36.62
± 17.20).
There was a significant difference in non
acceptance (t = 4.767, p < 0.01), goal
direction (t = 3.210, p < 0.01), impulse
control (t = 5.148, p < 0.01), strategies (t =
9.122, p < 0.01), lack of clarity (t = 3.523, p
= 0.01), and total emotional regulation (t =
5.950, p < 0.01).
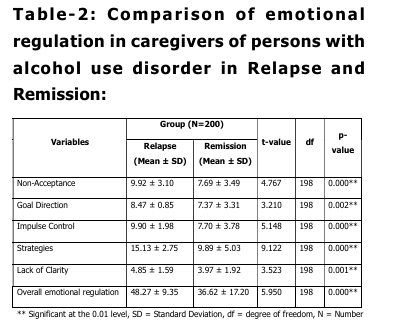
Table 3 shows a comparison of insomnia
among caregivers of persons with alcohol use
disorder in relapse and remission groups. The
mean score of insomnia was higher in the
relapse group (13.62 ± 6.28) compared to the
remission group (9.01 ± 9.74). The difference between the two groups was statistically
significant (t = 3.975, p < 0.01), indicating
that caregivers of patients in relapse
experienced greater insomnia symptoms than
those in remission.
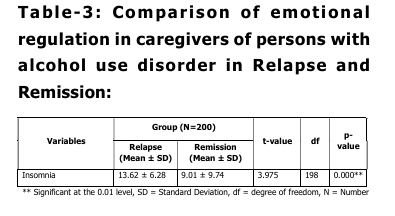
Table 4 shows that insomnia had a significant
positive correlation with all emotional
regulation variables. It was strongly
correlated with non- acceptance (r = 0.897, p
< 0.01), goal direction (r = 0.849, p < 0.01),
impulse (r = 0.877, p < 0.01), strategies (r =
0.892, p < 0.01), and lack of clarity (r =
0.898, p < 0.01). These findings indicate that
higher difficulties in emotion regulation were
strongly associated with greater insomnia
among caregivers of persons with AUD.
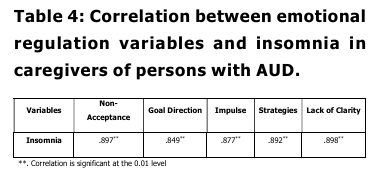
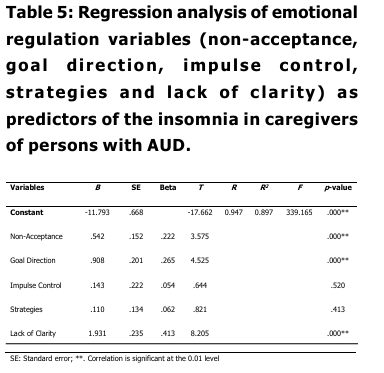
Table 5 The results of regression analysis
found that emotional regulation variables
were significant predictors of insomnia in
caregivers of persons with AUD (R² = 0.897,
F (5, 198) = 339.165, p < 0.001). Among the
predictors, non-acceptance (B = 0.542, p <
0.001), goal direction (B = 0.908, p < 0.001),
and lack of clarity (B = 1.931, p < 0.001) had
significant positive effects on insomnia, while
impulse control (B = 0.143, p = 0.520) and
strategies (B = 0.110, p = 0.413) were not
significant predictors. The adjusted R² value
of 0.897 indicates that these emotion
regulation variables together accounted for
about 89.7% of the variance in insomnia
among caregivers.
DISCUSSION
The present study found that caregivers of persons with AUD who were in relapse experienced significantly greater difficulties in emotion regulation across multiple domains, including non-acceptance, goal-directed behavior, impulse control, use of strategies, and emotional clarity, compared to caregivers of those in remission. This result is consistent with previous research indicating that relapse in AUD is associated with heightened family stress, increased caregiver burden, and greater emotional strain, which often manifest as difficulties in regulating emotions (Shetty et al., 2022; Rajpurohit et al., 2023). Similarly, Kaur et al. (2023) revealed that caregivers under chronic stress often experience a heavy care burden, which contributes to difficulties in managing expressed emotions. Other studies also indicate that caregivers of persons with substance use disorders frequently report higher levels of psychological distress, i mpaired coping, and limited emotion regulation strategies when faced with the unpredictability and challenges of relapse episodes (Koujalgi & Takkalaki, 2023; O’Farrell et al., 1998; Kumar et al., 2024). The present study found that caregivers of persons with AUD who were in relapse experienced significantly greater in insomnia compared to caregivers of those in remission. These findings are consistent with earlier research suggesting that caregiving for persons with chronic and relapsing conditions is associated with high physical burden and disrupted sleep (Sharma et al., 2021; Sen et al., 2016). Similarly, Goit et al. (2021) and Kalra and Tung (2024) also reported that caregivers of relapsing patients show poorer sleep and diminished physical quality of life compared to caregivers of remitted patients. Moreover, family members of people with alcohol dependence frequently experience sleep disturbances and reduced quality of life as a result of ongoing caregiving stress and uncertainty (Vadher et al., 2020; Gupta et al., 2015). Regression analysis further demonstrated that non-acceptance, goal direction, and lack of clarity were significant predictors of insomnia, explaining a substantial proportion of the variance in sleep disturbances. The strong positive correlation between emotional dysregulation and insomnia aligns with previous studies showing that poor sleep quality is closely linked with impaired emotional processing and regulation (Palmer & Alfano, 2017). Moos and Moos (2006) also reported that caregiving burden often leads to chronic insomnia, which in turn reduces emotional stability and resilience. Similarly, Cousino and Hazen (2013) highlighted that emotion regulation difficulties among caregivers can increase physical burden and lower coping capacity, particularly in high stress caregiving contexts.
The present study found that caregivers of persons with AUD who were in relapse experienced significantly greater difficulties in emotion regulation across multiple domains, including non-acceptance, goal-directed behavior, impulse control, use of strategies, and emotional clarity, compared to caregivers of those in remission. This result is consistent with previous research indicating that relapse in AUD is associated with heightened family stress, increased caregiver burden, and greater emotional strain, which often manifest as difficulties in regulating emotions (Shetty et al., 2022; Rajpurohit et al., 2023). Similarly, Kaur et al. (2023) revealed that caregivers under chronic stress often experience a heavy care burden, which contributes to difficulties in managing expressed emotions. Other studies also indicate that caregivers of persons with substance use disorders frequently report higher levels of psychological distress, i mpaired coping, and limited emotion regulation strategies when faced with the unpredictability and challenges of relapse episodes (Koujalgi & Takkalaki, 2023; O’Farrell et al., 1998; Kumar et al., 2024). The present study found that caregivers of persons with AUD who were in relapse experienced significantly greater in insomnia compared to caregivers of those in remission. These findings are consistent with earlier research suggesting that caregiving for persons with chronic and relapsing conditions is associated with high physical burden and disrupted sleep (Sharma et al., 2021; Sen et al., 2016). Similarly, Goit et al. (2021) and Kalra and Tung (2024) also reported that caregivers of relapsing patients show poorer sleep and diminished physical quality of life compared to caregivers of remitted patients. Moreover, family members of people with alcohol dependence frequently experience sleep disturbances and reduced quality of life as a result of ongoing caregiving stress and uncertainty (Vadher et al., 2020; Gupta et al., 2015). Regression analysis further demonstrated that non-acceptance, goal direction, and lack of clarity were significant predictors of insomnia, explaining a substantial proportion of the variance in sleep disturbances. The strong positive correlation between emotional dysregulation and insomnia aligns with previous studies showing that poor sleep quality is closely linked with impaired emotional processing and regulation (Palmer & Alfano, 2017). Moos and Moos (2006) also reported that caregiving burden often leads to chronic insomnia, which in turn reduces emotional stability and resilience. Similarly, Cousino and Hazen (2013) highlighted that emotion regulation difficulties among caregivers can increase physical burden and lower coping capacity, particularly in high stress caregiving contexts.
LIMITATIONS
This study has several limitations. First, the cross-sectional design limits the ability to establish causal relationships between emotion regulation difficulties and insomnia in caregivers. Second, the sample size, though adequate, was drawn from a specific geographic region, which may restrict the generalizability of findings to other populations. Third, self-report measures were used to assess emotion regulation and insomnia, which may be influenced by recall bias or social desirability. Fourth, other potentially relevant factors such as caregiver personality traits, coping styles, or the severity of the patient’s AUD were not assessed, which may have contributed to the observed outcomes.
This study has several limitations. First, the cross-sectional design limits the ability to establish causal relationships between emotion regulation difficulties and insomnia in caregivers. Second, the sample size, though adequate, was drawn from a specific geographic region, which may restrict the generalizability of findings to other populations. Third, self-report measures were used to assess emotion regulation and insomnia, which may be influenced by recall bias or social desirability. Fourth, other potentially relevant factors such as caregiver personality traits, coping styles, or the severity of the patient’s AUD were not assessed, which may have contributed to the observed outcomes.
CLINICAL IMPLICATIONS
This study shows that caregivers of persons with AUD, especially during relapse, face significant emotion regulation difficulties and insomnia. Clinically, this highlights the need for routine screening of caregivers for emotional distress and sleep problems. Interventions should combine emotion regulation training with sleep management strategies. Psychoeducation and counseling can reduce caregiver stress and stigma, while support groups and stress management programs can improve coping. Addressing caregiver well-being within treatment settings may also support better outcomes for patients with AUD.
This study shows that caregivers of persons with AUD, especially during relapse, face significant emotion regulation difficulties and insomnia. Clinically, this highlights the need for routine screening of caregivers for emotional distress and sleep problems. Interventions should combine emotion regulation training with sleep management strategies. Psychoeducation and counseling can reduce caregiver stress and stigma, while support groups and stress management programs can improve coping. Addressing caregiver well-being within treatment settings may also support better outcomes for patients with AUD.
CONCLUSION
The present study demonstrates that caregivers of persons with alcohol use disorder, particularly those in relapse, experience greater difficulties in emotion regulation and higher levels of insomnia compared to caregivers of persons in remission. Emotional dysregulation was strongly correlated with sleep disturbances, and specific domains such as non-acceptance, goal direction, and lack of clarity significantly predicted insomnia. These findings emphasize the need for targeted interventions focusing on emotional regulation skills and sleep management to reduce caregiver burden. Supporting caregivers in this way may not only improve their own health and well-being but also contribute to better recovery outcomes for persons with AUD
The present study demonstrates that caregivers of persons with alcohol use disorder, particularly those in relapse, experience greater difficulties in emotion regulation and higher levels of insomnia compared to caregivers of persons in remission. Emotional dysregulation was strongly correlated with sleep disturbances, and specific domains such as non-acceptance, goal direction, and lack of clarity significantly predicted insomnia. These findings emphasize the need for targeted interventions focusing on emotional regulation skills and sleep management to reduce caregiver burden. Supporting caregivers in this way may not only improve their own health and well-being but also contribute to better recovery outcomes for persons with AUD
REFERENCES
Ambekar, A., Agrawal, A., Rao, R., Mishra, A. K., Khandelwal, S. K., & Chadda, R. K. (2019). Magnitude of substance use in India, 2019. Ministry of Social Justice and Empowerment, Government of India. American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing. Bjureberg, J., Ljótsson, B., Tull, M. T., Hedman, E., Sahlin, H., Lundh, L. G., … & Gratz, K. L. (2016). Development and validation of a brief version of the difficulties in emotion regulation scale: the DERS 16. Journal of psychopathology and behavioral assessment, 38(2), 284-296. Cousino, M. K., & Hazen, R. A. (2013). Parenting stress among caregivers of children with chronic illness: A systematic review. Journal of Pediatric Psychology, 38(8), 809–828. Edwards, G., & Gross, M. M. (1976). Alcohol dependence: provisional description of a clinical syndrome. British medical journal, 1(6017), 1058. Gautham, M. S., Gururaj, G., Varghese, M., Benegal, V., Rao, G. N., Kokane, A., … & Shibukumar, T. M. (2020). The National Mental Health Survey of India (2016): Prevalence, socio-demographic correlates and treatment gap of mental morbidity. International Journal of Social Psychiatry, 66(4), 361-372. Glantz, M. D., Bharat, C., Degenhardt, L., Sampson, N. A., Scott, K. M., Lim, C. C., … & WHO World Mental Health Survey Collaborators. (2020). The epidemiology of alcohol use disorders cross-nationally: Findings from the World Mental Health Surveys. Addictive behaviors, 102, 106128. Goit, B. K., Acharya, B., Khattri, J. B., & Sharma, R. (2021). Burden and quality of life among primary caregiver of alcohol dependence syndrome. Am J Psychiatry Neurosci, 9, 1-6. Gross, J. J. (2015). Emotion regulation: Current status and future prospects. Psychological Inquiry, 26(1), 1–26. Gupta, A., Priya, B., Williams, J., Sharma, M., Gupta, R., Jha, D. K., … & Dhillon, P. K. (2015). Intra-household evaluations of alcohol abuse in men with depression and suicide in women: a cross-sectional community-based study in Chennai, India. BMC Public Health, 15(1), 636. Kalra, H., & Tung, S. (2024) A Call for Community Compassion: Recognizing and Supporting the Wellbeing of Caregivers in Alcohol Use Disorder Rehabilitation. Journal of Advance Research in Science and Social Science, 7(1), 123-132 Kalra, H., & Tung, S. (2024). Impact of Psychoeducational Classes on the Quality of Life of Alcohol Use Disorder Caregivers: A Comparative Analysis. International Journal of Indian Psych/logy, 12(3). Kaur, H., Mehta, S. G., Salvi, D., Kaur, S., Garg, S., & Warhade, M. (2023). A study of burden of care and expressed emotions i n the caregivers of patients with alcohol use disorder. International Journal of Medical Science in Clinica Research and Review, 6(3), 578–583. Koujalgi, S. R., & Takkalaki, M. S. (2023). Burden and coping among primary caregivers of persons with alcohol use disorder. Indian Journal of Psychiatric Social Work, 20-26. Kumar Goit, B., Acharya, B., Bahadur Khattri, J., & Sharma, R. (2021). Burden and Quality of Life Among Primary Caregiver of Alcohol Dependence Syndrome. American Journal of Psychiatry and Neuroscience, 9(1), 1 Kumar, S., Ravan, J. R., Thakur, B., & Banerjee, A. (2024). Factors related to high caregiver burden of wives of patients with alcohol dependence syndrome: A case-control study from Eastern India. Journal of Family Medicine and Primary Care, 13(10), 4628-4633. Liu, Y., Sun, Z., Wang, Q., Wu, K., Tang, Z., & Zhang, B. (2023). Contribution of alcohol use to the global burden of cirrhosis and liver cancer from 1990 to 2019 and projections to 2044. Hepatology international, 17(4), 1028-1044. McCurry, S. M., Logsdon, R. G., Teri, L., & Vitiello, M. V. (2007). Sleep disturbances in caregivers of persons with dementia: Contributing factors and treatment implications. Sleep Medicine Reviews, 11(2), 143–153. Moos, R. H., & Moos, B. S. (2006). Rates and predictors of relapse after natural and treated remission from alcohol use disorders. Addiction, 101(2), 212–222. O’Farrell, T. J., Choquette, K. A., & Cutter, H. S. (1998). Couples relapse prevention sessions after behavioral marital therapy for male alcoholics: outcomes during the t hree years after starting treatment. Journal of studies on alcohol, 59(4), 357-370. Orford, J., Copello, A., Velleman, R., & Templeton, L. (2010). Family members affected by a close relative’s addiction: The stress-strain-coping-support model. Drugs: Education, Prevention and Policy, 17(1), 36–43. Ortelli TA: Inside the National Institute on Aging . Am J Nurs. 2021, 121:70-1. Palmer, C. A., & Alfano, C. A. (2017). Sleep and emotion regulation: An organizing, integrative review. Sleep Medicine Reviews, 31, 6–16. Rajpurohit, S. S., Kaloiya, G. S., Sarkar, S., & Chadda, R. K. (2023). A prospective observational study of change in caregiver burden and psychological distress in caregivers of patients with alcohol dependence. Industrial Psychiatry Journal, 32(2), 266-272. Sen, S., Victor, R., & Saxena, K. (2016). Family burden in alcohol dependence: A study in north-eastern India. International Journal of Medical Science and Public Health, 5(11), 2402. Shetty, K. V., Manikappa, S. K., Murthy, S., Anjanappa, J., & Rawat, V. S. (2022). Expressed emotion among families of individuals with alcohol dependence syndrome: A pilot study. Annals of Indian Psychiatry, 6(4), 374-377. Vadher, S., Desai, R., Panchal, B., Vala, A., Ratnani, I. J., Rupani, M. P., & Vasava, K. (2020). Burden of care in caregivers of patients with alcohol use disorder and schizophrenia and its association with anxiety, depression and quality of l i fe. General psychiatry, 33(4), e100215.
Ambekar, A., Agrawal, A., Rao, R., Mishra, A. K., Khandelwal, S. K., & Chadda, R. K. (2019). Magnitude of substance use in India, 2019. Ministry of Social Justice and Empowerment, Government of India. American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing. Bjureberg, J., Ljótsson, B., Tull, M. T., Hedman, E., Sahlin, H., Lundh, L. G., … & Gratz, K. L. (2016). Development and validation of a brief version of the difficulties in emotion regulation scale: the DERS 16. Journal of psychopathology and behavioral assessment, 38(2), 284-296. Cousino, M. K., & Hazen, R. A. (2013). Parenting stress among caregivers of children with chronic illness: A systematic review. Journal of Pediatric Psychology, 38(8), 809–828. Edwards, G., & Gross, M. M. (1976). Alcohol dependence: provisional description of a clinical syndrome. British medical journal, 1(6017), 1058. Gautham, M. S., Gururaj, G., Varghese, M., Benegal, V., Rao, G. N., Kokane, A., … & Shibukumar, T. M. (2020). The National Mental Health Survey of India (2016): Prevalence, socio-demographic correlates and treatment gap of mental morbidity. International Journal of Social Psychiatry, 66(4), 361-372. Glantz, M. D., Bharat, C., Degenhardt, L., Sampson, N. A., Scott, K. M., Lim, C. C., … & WHO World Mental Health Survey Collaborators. (2020). The epidemiology of alcohol use disorders cross-nationally: Findings from the World Mental Health Surveys. Addictive behaviors, 102, 106128. Goit, B. K., Acharya, B., Khattri, J. B., & Sharma, R. (2021). Burden and quality of life among primary caregiver of alcohol dependence syndrome. Am J Psychiatry Neurosci, 9, 1-6. Gross, J. J. (2015). Emotion regulation: Current status and future prospects. Psychological Inquiry, 26(1), 1–26. Gupta, A., Priya, B., Williams, J., Sharma, M., Gupta, R., Jha, D. K., … & Dhillon, P. K. (2015). Intra-household evaluations of alcohol abuse in men with depression and suicide in women: a cross-sectional community-based study in Chennai, India. BMC Public Health, 15(1), 636. Kalra, H., & Tung, S. (2024) A Call for Community Compassion: Recognizing and Supporting the Wellbeing of Caregivers in Alcohol Use Disorder Rehabilitation. Journal of Advance Research in Science and Social Science, 7(1), 123-132 Kalra, H., & Tung, S. (2024). Impact of Psychoeducational Classes on the Quality of Life of Alcohol Use Disorder Caregivers: A Comparative Analysis. International Journal of Indian Psych/logy, 12(3). Kaur, H., Mehta, S. G., Salvi, D., Kaur, S., Garg, S., & Warhade, M. (2023). A study of burden of care and expressed emotions i n the caregivers of patients with alcohol use disorder. International Journal of Medical Science in Clinica Research and Review, 6(3), 578–583. Koujalgi, S. R., & Takkalaki, M. S. (2023). Burden and coping among primary caregivers of persons with alcohol use disorder. Indian Journal of Psychiatric Social Work, 20-26. Kumar Goit, B., Acharya, B., Bahadur Khattri, J., & Sharma, R. (2021). Burden and Quality of Life Among Primary Caregiver of Alcohol Dependence Syndrome. American Journal of Psychiatry and Neuroscience, 9(1), 1 Kumar, S., Ravan, J. R., Thakur, B., & Banerjee, A. (2024). Factors related to high caregiver burden of wives of patients with alcohol dependence syndrome: A case-control study from Eastern India. Journal of Family Medicine and Primary Care, 13(10), 4628-4633. Liu, Y., Sun, Z., Wang, Q., Wu, K., Tang, Z., & Zhang, B. (2023). Contribution of alcohol use to the global burden of cirrhosis and liver cancer from 1990 to 2019 and projections to 2044. Hepatology international, 17(4), 1028-1044. McCurry, S. M., Logsdon, R. G., Teri, L., & Vitiello, M. V. (2007). Sleep disturbances in caregivers of persons with dementia: Contributing factors and treatment implications. Sleep Medicine Reviews, 11(2), 143–153. Moos, R. H., & Moos, B. S. (2006). Rates and predictors of relapse after natural and treated remission from alcohol use disorders. Addiction, 101(2), 212–222. O’Farrell, T. J., Choquette, K. A., & Cutter, H. S. (1998). Couples relapse prevention sessions after behavioral marital therapy for male alcoholics: outcomes during the t hree years after starting treatment. Journal of studies on alcohol, 59(4), 357-370. Orford, J., Copello, A., Velleman, R., & Templeton, L. (2010). Family members affected by a close relative’s addiction: The stress-strain-coping-support model. Drugs: Education, Prevention and Policy, 17(1), 36–43. Ortelli TA: Inside the National Institute on Aging . Am J Nurs. 2021, 121:70-1. Palmer, C. A., & Alfano, C. A. (2017). Sleep and emotion regulation: An organizing, integrative review. Sleep Medicine Reviews, 31, 6–16. Rajpurohit, S. S., Kaloiya, G. S., Sarkar, S., & Chadda, R. K. (2023). A prospective observational study of change in caregiver burden and psychological distress in caregivers of patients with alcohol dependence. Industrial Psychiatry Journal, 32(2), 266-272. Sen, S., Victor, R., & Saxena, K. (2016). Family burden in alcohol dependence: A study in north-eastern India. International Journal of Medical Science and Public Health, 5(11), 2402. Shetty, K. V., Manikappa, S. K., Murthy, S., Anjanappa, J., & Rawat, V. S. (2022). Expressed emotion among families of individuals with alcohol dependence syndrome: A pilot study. Annals of Indian Psychiatry, 6(4), 374-377. Vadher, S., Desai, R., Panchal, B., Vala, A., Ratnani, I. J., Rupani, M. P., & Vasava, K. (2020). Burden of care in caregivers of patients with alcohol use disorder and schizophrenia and its association with anxiety, depression and quality of l i fe. General psychiatry, 33(4), e100215.
Conflict of interest: None
Role of funding source: None
