
Indian Journal of Health Social Work
(UGC CARE List Journal)
USE OF MINDFULNESS BASED STRESS REDUCTION ON
INDIVIDUALS WITH OPIOID ADDICTION
Laxmi Narayan Rathore
Associate Prof, Dept of Clinical Psychology, Mizoram University,
Aizawl, Mizoram-796004
Correspondence: Laxmi Narayan Rathore, e-mail: laxminarayan21@rediffmail.com
ABSTRACT
Keywords: Substance Use, Craving, Opioid, Mindfulness, MBSR.
Submitted: 18.09.2025 Revised: 24.10.2025 Accepted: 12.11.2025 Published: 28.01.2026
Throughout the world, Opioid addiction continues to represent a significant health crisis, with less than 15% of such individuals seek formals treatments (Mutumba et al, 2021), which is often discontinued, leading to relapses. One of the main reasons for relapse is that of ‘craving’ in individuals with opioid use. Craving, which is the subjective experience of an urge or desire to use a substance (Kozlowski et al, 1987), has been associated with activation of brain networks, l eading to its conceptualization as a motivational and emotional state of an individual. The relevance of craving in clinical field is emphasized by its inclusion as one of the main diagnostic criteria for ‘Dependence Syndrome’ for Substance Use Disorder (SUD), in International Classification of Diseases-10 (ICD-10), among other factors. It has been well documented that, it’s often the mismanagement of the desire (craving) that leads to the individuals to continue with intake of the psycho-active substance especially in case of opioid addiction. As such, opioid and i ts derivates were known to cause physiological and psychological dependency, in the individual quite rapidly, in comparison to the forms of psychoactive substance (Sadoock et al, 2015). Thus, it’s the unmanaged craving behavior, which plays a vital role in the maintenance of the substance intake, there-by increasing the substance use period and consequentially leading to more neuro-chemical disturbances in the individual. This leads to the increase in burden, not only on the healthcare systems but also on the society. Thus, for effective management in case of opioid addiction, minimizing and managing craving behavior becomes essential. Traditionally, pharmacological methods were in to practice for addressing the craving issues, in substance addiction population. Some of the molecules, used, were quite effective in minimizing the severity of craving in individuals OUD. One such treatment strategy is opioid substitution therapy (OST), which basically helps the abusers, to substitute for the neutral agent having lesser addictive properties, there-by preventing the individual from more harmful effects of opioid substance. Over the years efforts were made to look for alternative modes of intervention for management of craving behavior, which have a long lasting effectiveness. Apart from other alternative techniques being explored, over the years, mindfulness-based interventions were also used. Mindfulness, broadly defined as “the awareness that emerges by paying attention on purpose, at present moment, and non-judgmentally to the unfolding of the experience, from moment to moment” (Kabat-Zinn, 1992). Prior studies involving mindfulness does observed that mindfulness is effectively associated with stress management & enhancing resilience (Chambers et al, 2018) ; positivity (Jain et al, 2007), improving anxiety and depressive symptoms (Gu et al, 2015), Self-compassion (Keng et al, 2011) among others. From a conceptual understanding, ‘Mindfulness’ holds significance in shifting the mental focus of the individual to the present moment happenings in his life, without becoming reactive towards it. With non-judgmental awareness to the present moment, the individual could develop ‘equanimity of mind’ (Hart, 1987). This stability of mind (equanimous mind) helps the i ndividual to observe the physiological sensations happening in his body, in a non reactive, non-judgmental manner, leading to the development of an understanding about the ‘impermanence’ nature of all physiological sensations. With practice, there is a shift in the individual behavior and attitude, from reactive to non-reactive, and the understanding about ‘impermanence’ nature of events, becomes more consolidated. Such developments could certainly help the individual to have a more peaceful state throughout. In substance addiction, the ‘craving state’ is usually characterized by physiological and psychological agitation, and under its influence, the individual usually gives up to the desire and continues/initiate his substance intake, leading to continuity of substance addiction and/or relapse state. Therefore interventions/techniques based on ‘mindfulness’ could prove to be useful in addressing the craving issue, in substance addiction. However, effectiveness of mindfulness based interventions, in managing the craving behavior in individuals with substance use has not been explored substantially. Thus this study has been planned. The broad aim of this cross-sectional study was to examine the role of MBSR in managing the carving experiences of male individuals with OUD, which could help in understanding its usefulness in addressing craving issues in this population.
The following objective were framed for the study: To explore the usefulness of Mindfulness Based Stress Reduction in managing the craving among individuals with Opioid addiction.
Mindfulness Based Stress Reduction will have no effect on craving behavior of individuals with Opioid addiction.
Inclusion Criteria
◾Male Aged between 18-45 years.
◾Participants with Opioid Dependence as per ICD-10.
◾Having at least Primary level education
◾Exclusion Criteria
◾Persons with Multiple Drug/Substance abuse except nicotine use.
◾ Any Co-morbid Major Psychiatric/ Neurological/ medical disorders.
◾Any significant Physical Disability/ Handicap
Study design- Pre-Post with Control design
2. WHO-ASSIST V 3.0:
The World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (WHO-ASSIST), is a widely accepted tool used in health care settings, particularly in community care, to screen out individuals for substance abuse and risk behaviors related with substance intake, such as like alcohol, nicotine and other substances /drugs. Version 3.0 was used in this study. The responses could be collected using an interview method. It has acceptable validity as a screening tool in mental health settings.
Developed by McHugh et al (2021), this scale of craving is a self- reported, 3-item tool to assess the severity of craving experience in an individual. This scale enjoys a high concurrent and discriminate validity.
Developed by May et al (2014), CEQ is a brief and psychometrically sound measure of measuring desires (craving). It is based on Elaborated Intrusion (EI) theory model. It is widely used as a short measure of assessing the craving tendencies among participant for a particular substance and is answered on a 10 point scale from ‘not at all’ to ‘extremely’. It can be self-administered or administered by a health care worker/ clinician.
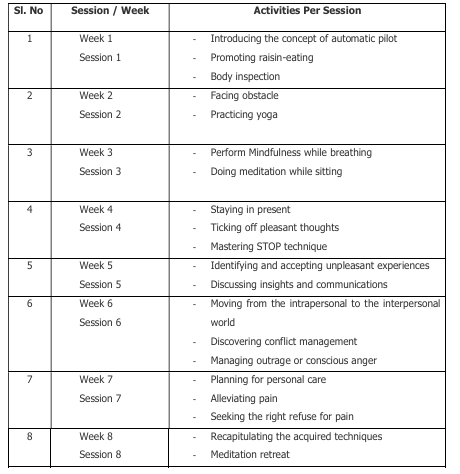
Mindfulness Based Stress Reduction (MBSR) as developed by John Kabat-Zinn, was used in this study as an intervention tool. It consists of 08 weekly sessions. The broad outline of each session is depicted below:
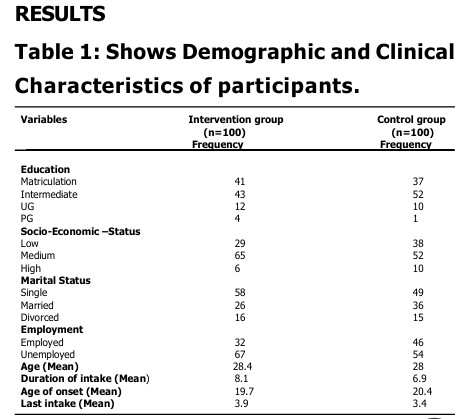
The current study, following a pre-post with control design, explores the effectivenesss of MBSR program on craving in a sample of male adults (N=200) with Opioid dependence. Participants, aged between 18-45 years, were recruited from de-addictions centers in Aizawl city, using convenient sampling method, after Institutional Ethics Committee (IEC) approval. Upon, signing the informed consent, pre diagnosed participants having Opioid dependence as the primary diagnosis, were screened on ASSIST V 3.0 to rule out poly substance use. Those, who passed screening, were enrolled for the study and were allocated in to two groups, Intervention and Control, in equal numbers, following draw of-lots method. The intervention group participants were provided eight sessions of MBSR program as developed by Jon Kabat Zinn, at a frequency of one session per week. All activities were conducted at spacious hall inside the centers itself and the participants were encouraged to practice them, for remaining 6 days of weeks, under observation from the staff at centre. However they were allowed to participate in other activities at centers as well, such as games, pastoral counseling, prayer, recreational and gardening activities, as per their centre routine, during their stay at de-addiction centers. The participants of control group were not provided any session of MBSR, they were kept under observation only. During the entire process of data collection (3 months), all the participants of both groups were allowed to continue with their ‘Treatment-As Usual’ (TAU). Participants were assessed on Opioid Craving Scale (OCS) and Craving Experience Questionnaire (CEQ) to measure Craving. The assessments on outcome measures (CEQ & OCS) were obtained at three different stages; baseline (before MBSR training- First), post-intervention (after 8 week of MBSR training-Second) and at follow up (after one month of second assessment Third) for all participants
Following the data collection process, obtained data was analyzed using SPSS-29 statistical software for windows. Non-parametric analysis was carried out for analyzing the data, as obtained data does not follow measures of normality.
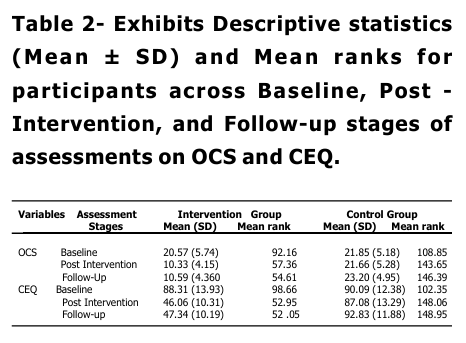
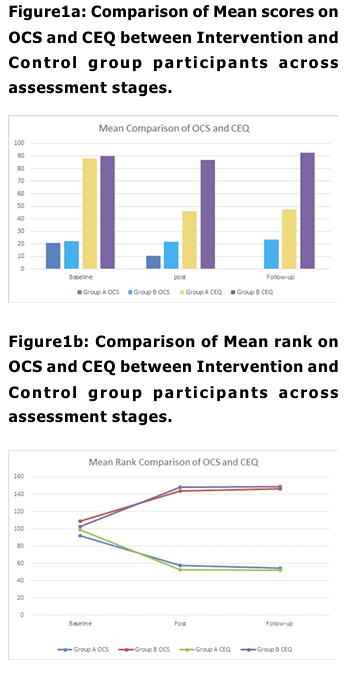
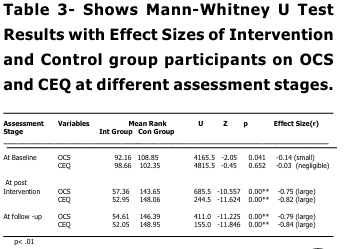
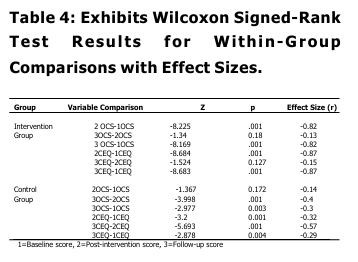
The study involved a total of 200 male participants with opioid addiction, taken from various de-addiction centers, were they are receiving treatment under supervision of qualified mental health professionals. Elevated CEQ and OCS scores, indicated strong craving at baseline in both groups with small to negligible effect sizes (Mr=0.07); and negligible effect size (-0.01) for OCS & CEQ respectively, pointing to minimal practical significance between groups. Conclusively, groups indicate no significant difference between them on CEQ and OCS at baseline stage. These finding goes in line with existing literature, which explains that persons with substance abuse are mostly influenced by external cues in the surroundings, and there by it maintain their substance taking tendencies. A noticeable decline in mean scores among intervention group participants, indicated significant improvements in their craving at post intervention stage, which also witnessed significant group difference (p<0.01) in terms of their desire for opioid intake (OCS & CEQ). This finding is significant, as both groups participants were not only receiving similar pharmacological treatment (OST) at their de addiction centers, but also sharing matched socio-demographic background and following similar routines at de-addiction centers like, games, pastoral counseling, prayers and gardening during their course of stay at their de-addiction centers. Thus, the group which has received 8 weeks of MBSR training is more instrumental in bringing significant decline in craving behaviors, as a whole. MBSR program basically aims to develop a sense of mindfulness awareness, related with present, non-judgmentally, leading to equanimity of mind. This, not only helps the learner to develop awareness and complete focus with regard to present events but with a non judgmental attitude, but also develops an understanding about impermanence of events. Such changes, in SUD, could not only, had been helpful in recognizing that physiological/ psychological changes, that fueled the desire to take a substance will automatically cease away after some time and also due to the enhanced awareness about present event, the participant was least bothered with past/ futuristic thinking related with substance use, their-by modifying the substance taking behavior. The probable mechanism for this change lies in the various ‘mindful’ activities that were a part of MBSR training sessions spreading over 8 weeks. Such activities, like yoga, raisin eating, meditation, breathing exercises body-scaning etc, have the potential of developing an understanding of the concept of ‘impermanence’ of physiological sensations/ drives/thoughts etc, there-by leading to the attainment of ‘equanimous mind’ in the individual (Hart, 1987) . With ‘equanimity of mind’, the psychological/physiological yielding (craving) to take substance (opioid), gets delayed or take a back seat, gradually leading towards the elopement of same. So, while established treatment procedures, may decrease the craving experience cross sectionally, mindfulness-based training adds extra long-term benefits. Post-intervention, larger reduction of craving severity, in the Intervention group is in line with previous research that shows mindfulness-based interventions enhance emotion regulation and impulse control, key factors in addictive behaviors (Bowen et al., 2014), make aware of craving thoughts and sensations without acting on them. Also the significant reduction of Craving in Intervention group may reflect the intervention’s emphasis on acceptance and distress tolerance; skills that help individuals cope with withdrawal symptoms and cravings without using (Witkiewitz et al., 2013). Between group differences on OCS and CEQ is also maintained on effect size analysis, as well, with OCS (-0.75) & CEQ (-0.82) demonstrated significantly large effect sizes on both measures (r range:0.64-0.82), i ndicating profound between group differences related with craving experiences at post training (after 8 weeks), suggesting substantial differential treatment response. Broadly, this could also aligns with neuro cognitive research indicating that mindfulness disrupts automatic craving responses by reducing activation in craving-related brain regions (Zgierska et al., 2019). Mean scores, expanded effect sizes and significant group differences ( p<0.01) at follow-up stage for OCS and CEQ continue to support better scores among intervention group participants suggested that post mindfulness training changes were not only substantial but maintained over time, i ndicated by reduced craving. These observations, depicts the effectiveness of MBSR in bringing a long lasting change in the attitude of the learner that could be maintained over time, were consistent with previous findings (Bowen et al, 2009) highlighting applicability of mindfulness-based intervention as an adjunct therapy, if not mono-therapy, in addressing craving issues in OUD. With-in group analysis also supports robust treatment effect and clinically relevant changes in intervention group, indicated significant differences in pre-post data comparison, on CEQ and OCS, which maintained during follow-up and post intervention analysis. However, for non MBSR group, fewer changes suggested natural variability rather than systematic improvement. These findings reinforce the efficacy of the MBSR intervention in reducing psychological distress and enhancing adaptive functioning compared to the control condition. Though the study exhibits promising findings, but also has certain limitations. The major limitation relates with its generalization, study findings cannot be generalized on females and t he study has limited Cross-cultural applicability of findings. The study fails to address the influence of personal factors in craving management in substance use.
Study concluded that mindfulness-based intervention was effective in addressing craving tendencies in individuals with Opioid dependence. These findings contribute to the growing evidence base supporting the use of mindfulness-based interventions as a promising approach in craving management in Opioid addiction, their-by establishing MBSR as an alternative treatment mode in this population.
Bowen, S., et al. (2014). Relative efficacy of mindfulness-based relapse prevention, standard relapse prevention and treatment as usual for substance use disorders: a randomized clinical trial. JAMA Psychiatry, 71(5), 547-556. Chambers, R., Gullone, E., & Allen, N. B. (2018).Mindful emotion regulation: an integerative review. Clinical Psychology Review, 29 (6), 560-572. Fleischman, P. R. (1986).The Therapeutic Action of Vipassana and Why I Sit, Buddhist Publication Society, Kandy, Sri Lanka. Fleischman P. R. (1991) Vipassana Meditation: Healing the Healer and The Experience of Impermanence. Vipassana Research Institute, Igatpuri, India. Goleman, D. (1977). Meditation and Consciousness: An Asian Approach to Mental Health. American Journal of Psychology, 30: 41-54. Goenka, S. N. (1988). Altruism: Quintessence of Religion, in: Issues of Biomedical Ethics- Proceedings of the Festival of Life International Congress, December Bombay; Editors: Vas C J & de Souza E J; McMillan India Ltd., Delhi, 95-102. Gu, J., Strauss, C., Bond, R., & Cavanagh, K. (2015). How do mindfulness- based congnitive therapy and mindfulness based stress reduction improves mental health and well being? A systematic review and meta-analysis of mediation studies. Clinical Psychology Review, 37, 1-12. Hart, W. (1987). The Art of Living: Vipassana Meditation as taught by S.N. Goenka. Harper and Row, New York. Jain, S., et al. (2007). A randomized controlled trial of mindfulness meditation versus relaxation training: effects on distress, positive states of mind, rumination and distraction. Annals of Behavioral Medicine, 33(1), 11-21. Kabat-Jinn, J., et al. (1992). Effectiveness of a Meditation based stress reduction program in the treatment of anxiety disorders. American Journal of Psychiatry, 149 (7), 936-945. Keng, S.L., Smoski, M.J., & Robins, C.J. (2011). Effects of mindfulness on psychological health: a review of empirical studies. Clinical psychology review, 31(6), 1041-1056. Koziowski, L.T. & Wilkinson, D.A. (1987). Use and misuse of the concept of craving by alcohol, tobacco and drug researchers. British Journal of Addiction. 1987, 82(1), 31-36. Koob, G. F. & Volkow, N. D. (2016). Neurobiology of addiction: a neuropsychiatry analysis. The Lancet Psychiatry, 3(8):760-763. May, J., et al. (2014). The craving experience questionnaire: a brief, theory-based measure of consummatory desire and craving. Addiction. 109(5):728-35. doi: 10.1111/add.12472. Epub 2014 Feb 16. PMID: 24400950. Mutumba, M., et al. (2021). A mindfulness based, streaa and coping model of craving in methamphetamine users. PLoS ONE 16(5):e0249489. https:// doi.org/10.1371/journal.pone.0249489. McHugh, R.K., Trinh, C.D., Griffin, M.L., Weiss, R.D. (2021). Validation of the craving scale in a large sample of adults with substance use disorders. Addictive Behaviors, 113 (2). Naqvi, N. H., Gaznick, N., Tranel, D., Bechara, A. (2014). The insula: a critical neural substrate for craving and drug seeking under conflict and risk. Annals of the New York Academy of Sciences, 1316 (1), 53-70. Sadock, B., et al. (2015). Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. Lippincott Williams & Wilkins. Vipassana Research Institute. (1990). A Reader: International Seminar on Vipassana Meditation and Health. Igatpuri, India. Witkiewitz, K., et al. (2020). Mindfulness based relapse prevention for alcohol use disorders: findings from a randomized controlled trial. Journal of Consulting and Clinical Psychology, 88(6),537-552. World health Organization. (2010). The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST). WHO team, Geneva. Zgierska, A., et al. (2019). Mindfulness meditation for substance use disorder: a systematic review. Substance Abuse, 40 (2), 178-194.
This study is a part of the approved research project (ID:2022-1439) and was fully funded by ICMR-DHR, Govt of India (File.No.11012/27/2023-GIA/HR) under its Grant-in-aid (GIA) Scheme of the Department of Health Research for ‘Inter Sectoral Convergence & Coordination for Promotion and Guidance on Health Research approval to the research project entitled “Using Mindfulness Component of Vipassana Meditation as An Adjunct Treatment Modality in The Treatment of Persons with Opioid Addiction – An Exploratory Study from Mizoram. Project Granted to Principal Investigator-Dr. Laxmi Narayan Rathore, Mizoram University. The author wishes to acknowledge the financial support granted by the funding agency (ICMR-DHR, Govt. of India) and also to all the participants of the study for their valuable time and effort.
Conflict of interest: None
