
Indian Journal of Health Social Work
(UGC CARE List Journal)
PALLIATIVE CARE IN INDIA: THE ROAD AHEAD
Gayathri P Nair1 & Sabu P Thomas2
Correspondence: Gayathri P Nair, e-mail: gayathrinair097@gmail.com
ABSTRACT
As the prevalence of Non-Communicable Diseases (NCDs) rise worldwide and more patients
need long-term care for chronic diseases, palliative care is becoming more and more important.
Palliative care is basically to provide physical, social, emotional comfort for persons dealing with
life threatening illnesses. It is helpful for both patients and care givers in managing symptoms
including the pain relief. Even though the services of palliative care has been widely acknowledged
across the globe, the developing countries like India lacks a lot in providing a total care for the
individuals in need of palliative care. This article tries to explore the development of palliative
care in India along with the critical gaps such as lack of training and capacity building,
unawareness of pc among the public as well as persistent barriers to the adequate availability
and use of morphine and other essential pain-relieving medications. By synthesizing recent
literature and policy developments, this paper emphasizes the need for effective national strategies
to address these gaps, improve service delivery, and enable all Indians to access equitable
palliative care. The discussion emphasizes the importance of integrating palliative care within
systemic healthcare delivery, committing to workforce capacity development, and amending
regulatory barriers to address some of the current challenges to service provision.
Keywords: Palliative care in India, Emergence of Palliative care, Service gaps
Submitted: 10.09.2025 Revised: 16.10.2025 Accepted: 06.11.2025 Published: 28.01.2026
How to cite this article: Nair, G. P., & Thomas, S. P. (2025). Palliative care in India: The
road ahead. Indian Journal of Health Social Work, 7(2), 42-52.
INTRODUCTION
As the prevalence of Non-Communicable
Diseases (NCDs) rises worldwide and more
patients need long-term care for chronic
diseases, palliative care is becoming more
and more important (Murray & Lopez,
1997).The World Health Organization defines
palliative care as ‘an approach that improves
the quality of life of patients and their families
facing the problems associated with life
threatening illness, through the prevention and relief of suffering. Palliative care services
are crucial for providing patients and their
families with comprehensive treatment where
the prevalence of chronic illnesses is
significant. The diagnosis should be
accompanied by the field of palliative care. It
i s designed to provide physical, social,
mental, and spiritual comfort and respite to
people who have been diagnosed with any
kind of debilitating illness or life-limiting
condition. Palliative care is not just for dying
or lessening the process of dying; it can also
be given at the time of diagnosis. Palliative
care is also not about end-of-life care, despite
the common misconception that it is solely
provided during these times.
Just 14% of people worldwide have access to
specialist palliative care(Palliative Care, n.d.)
An estimated 56.8 million individuals
worldwide, including 25.7 million nearing the
end of their lives, need palliative care each
year. Over 61 million people annually suffer
from illnesses associated with suffering that
may be significantly decreased with Palliative
Care, according to estimates from the Lancet
Commission on Global Access to Palliative
Care and Pain Relief (henceforth referred to
as The Lancet Commission). At least 80% of
patients cannot afford even the most basic
PC therapy, such as painkillers (Knaul et al.,
2018). Over the past few decades, there have
been significant advancements in the global
need for palliative care, but many gaps remain
to be identified and filled(Sepúlveda et al.,
2002) Palliative care can be given in
conjunction with curative treatment and is
suitable at any age and stage of a serious
illness. About 25·5 million of 56·2 million
people who died in 2015 experienced serious
health-related suffering, and another 35·5
million experienced serious health-related
suffering due to life-threatening and life
limiting conditions(Knaul et al., 2018) For many
conditions, palliative care is necessary.
Cardiovascular disorders (38.5%), cancer
(34%), chronic respiratory diseases (10.3%),
AIDS (5.7%), and diabetes (4.6%) account for
the bulk of adults who require palliative
care(Palliative Care, n.d.) Numerous other
illnesses, such as congenital defects, multiple
sclerosis, Parkinson’s disease, rheumatoid
arthritis, renal failure, chronic liver disease,
neurological disorders, dementia, and drug
resistant tuberculosis, may also necessitate
palliative care. Two of the most common and
dangerous symptoms that individuals in need
of palliative care encounter are pain and
breathing difficulties. For instance, 67% of
patients with cardiovascular illness or chronic
obstructive pulmonary disease and 80% of
patients with cancer or AIDS may have
moderate to severe pain in their final days.
Opioids are necessary for controlling.
India is a country which has one billion
populations which is about the world’s one
sixth of total population. So it is extremely
difficult and challenging at the same time to
provide care for the individuals who are in
need of palliative care with respect to its
enormous population. Initially palliative care
was all about treating cancer and treating
people with end of life care. During the 1990s
like in other developing nations, cancer
awareness had been growing in India.
According to estimates, there are roughly 0.5
million cancer cases in the nation at any one
moment, with over 0.5 million new cases
added annually(Vijayaram, 1993). Only
palliative care was feasible because most of
these cancer patients arrive for treatment at
an advanced stage of the illness. The
treatment facilities were too few to meet the
needs and were mostly limited to urban areas.
Facing all these challenges and overcoming
from this scenario, Palliative care field has
transformed drastically in India. It has been
available in India for roughly 20 years, despite
i ts restricted reach. Numerous factors,
i ncluding population density, poverty,
geographic diversity, restrictive policies regarding the prescription of opioids,
workforce development at the base level, a
lack of institutional interest in palliative care,
and a limited national palliative care policy,
were impeding the growth of palliative care
in India(Khosla et al., 2012)
With all these hindering factors existed, India
gave birth to palliative care in the name of
Santhi Avedana sadhan, Mumbai in the year
1987, which was a hospice(Rajagopal, n.d.
a) Within the coming years it also had
established two other centres in Goa and
Delhi. Indian Association of Palliative care and
Pain and palliative care society in the years
1993-94 took another major transformation
in the field of palliative care in India. A
number of additional palliative care projects
were launched during the course of the
following few years, in the later half of the
1990s, including the Guwahati Pain and
Palliative Care Society in Assam. The
Karunasraya Hospice in Bangalore, the
Lakshmi Palliative Care Trust in Chennai,
Jivodaya Hospice in Chennai, and Cansupport
in Delhi also established in the meantime.
Palliative care was offered by a few regional
cancer centers, such as those in Trivandrum,
Bangalore, and Delhi, which already
established pain management programs.
Despite the addition of a few centers annually,
the growth was constrained by the size of the
Indian population. Along with that the
Neighborhood Network in Palliative care model
was flourished well in the Northern states of
Kerala, in India(Kumar, 2007). As part of the
lancet commission as well as the World Health
Organization ‘s emphasis on the need of
integrating palliative care into the National
health system of the countries, India also had
included palliative care in the National Health
Policy 2017(National Health Policy 2017 .Pdf,
n.d.).Despite all these notable progresses and
changes in the field of palliative care since
then, India still faces major challenges and
gaps in providing effective palliative care
treatment to its huge population who are in
need of the same. According to the Lancet
Commission report, 7 million Indians require
palliative care(Ghoshal, Joad, et al.,
2022).There is a pressing need to guarantee
proper palliative care service due to an aging
population, rising morbidity and mortality from
cancer, and other non-communicable
diseases. This article critically reviews the
literatures published between the year 2015
to 2025, to evaluate the evolution, policy
changes, gaps and other progresses in
palliative care in India.
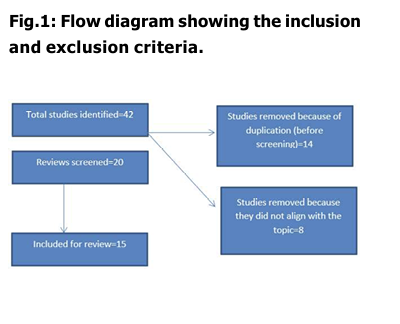
METHODOLOGY
A comprehensive review of literatures were
conducted utilizing multiple sources which
includes governmental documents, policy
documents of various organizations both of
global and national importance and also
selected articles from various databases
namely PubMed, Jstor ,and scopus. Keywords
like “palliative care”, “evolution of palliative
care in India” were used. Studies conducted
in India was only included.
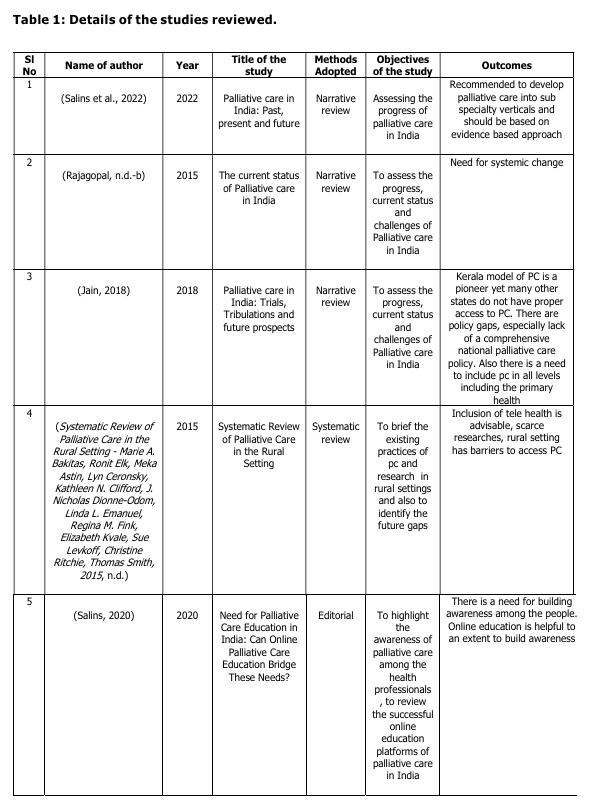
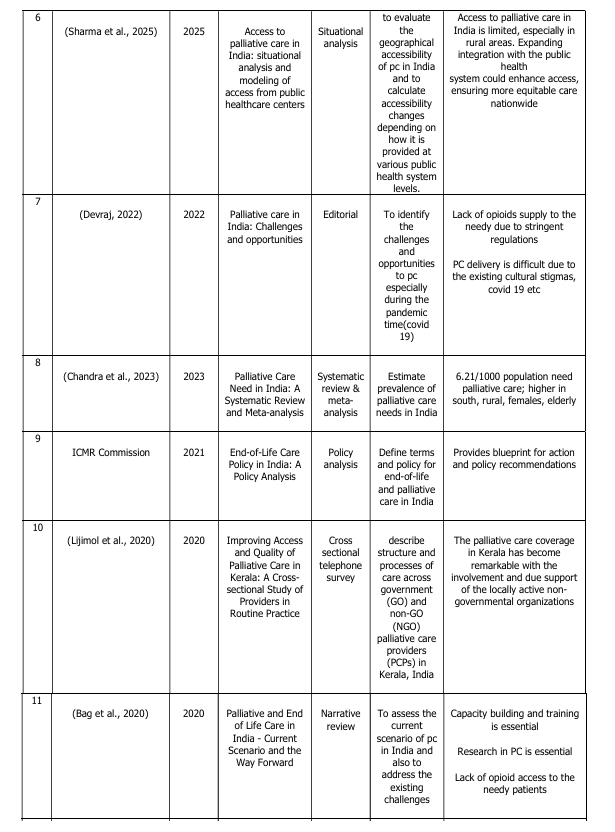
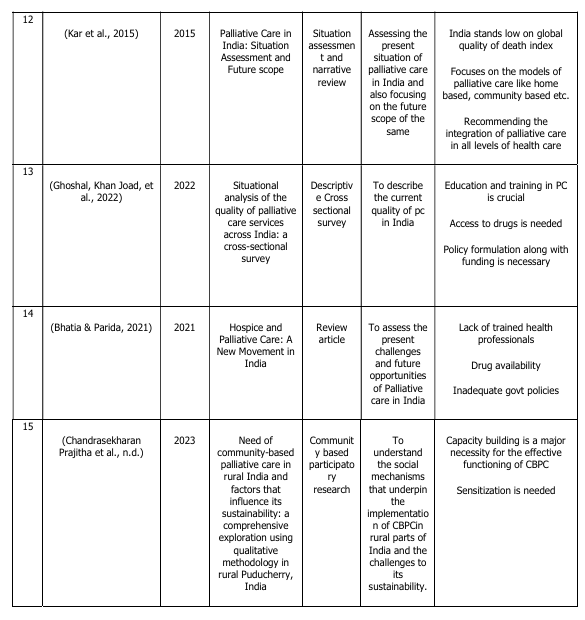
FINDINGS
Overview of the studies
1. Lack of awareness on palliative care among the public
2. Capacity building is required
3. Lack of drug availability
4. Integration of palliative care into all the levels of health
5. Policy recommendation including a comprehensive national policy for palliative care
Lack of awareness on palliative care among the public
Dying and end-of-life care were central to the
palliative care philosophy. Many
improvements have been made to this field
as a result of the ongoing efforts of the
government, non-governmental organizations,
and other stakeholders. Major policy
implementations on palliative care have
emerged as milestones. The development,
present situation, and deficiencies in India’s
palliative care system were the main topics
of this study. Lack of public awareness of palliative care is the main subtheme that
emerged; it is evident from the evaluated
studies that the public does not have adequate
knowledge about palliative care. Some health
care providers are even ignorant (Sujatha &
Jayagowri, 2017).According to a study
(Ramasamy Venkatasalu et al., 2018), the
public’s perceptions of palliative care are
influenced by the cultural, social, and religious
spheres. Additionally, the study discovered
that nurses require additional awareness and
specialized skills to manage patients who
require palliative care. However, it is clear that
public awareness is extremely low when
contrasting it with professionals’ awareness
(Gopal & Archana, n.d.)
Awareness and knowledge need to be
improved in palliative care especially among
general population hence utilization of
palliative care could be maximized thereby
providing a good quality of life by the sufferers
and their families until the end of the journey
Capacity building
Capacity building from the grass root level is
very essential to strengthen the palliative care
services across. Building the capacity of
palliative care in ASHA (Accredited Social
Health Activist) workers is crucial for
i mproving community-based healthcare
delivery in India. ASHA workers are often the
first point of contact in rural and underserved
areas. They play a key role in identifying
patients with life-limiting illnesses, providing
basic symptom management, and offering
psychosocial support. Training programs that
f ocus on palliative care principles,
communication skills, home care techniques,
and referral systems can help them provide
compassionate and comprehensive care.
Providing ASHAs with knowledge and practical
skills improves early identification and
continuity of care. It also raises awareness
and acceptance of palliative care at the
community level. And for care givers, capacity
building is very crucial in ensuring the quality
of care for the patients specifically in home
based care. The care givers require nursing
skills, safe medication handling, pain
management etc. Improving their skills not
only raises the quality of care but also creates
a more caring and lasting home care
environment.
A study conducted in Canada developed a
theoretical model that conceptualizes the
process of developing palliative care
programs in rural areas in four sequential
phases like the antecedent, catalyst, creating
the team, and growing the program(Lou
Kelley, 2007) which improves the access of
palliative care especially for the ageing
population. So the community also requires
the ability to deal with the pc recipients. Along
with that the doctors, nurses, volunteers and
social workers who plays a vital role in
providing care must take part in various
courses, workshops offered by NGOs, health
department, other stakeholders. Many studies
emphasizes that palliative care should be part
of undergraduate (UG) and postgraduate (PG)
medical programs. This integration will help
future healthcare professionals gain the skills
and knowledge needed to care for patients
with life-limiting illnesses.
Strengthening Palliative Care through
Integration across Health Systems and
Ensuring Essential Drug Availability
Palliative care must be strengthened by being integrated into the health system at all levels and by guaranteeing that necessary drugs, such as opioids, are available for symptom control and pain management. This entails educating the public, training medical personnel, and collaborating between primary care and specialized palliative care physicians. Palliative care must also be incorporated into national plans and goals, as well as into financial methods. India had reported some medical use of morphine for decades; it was used mainly in injection form in hospitals to relieve post-operative pain (Joranson et al., 2002).Later with the advancement of time opioid availability started increasing with the influence of various policy regulations. Access to pain-relief medications remains limited, even though the WHO includes them on its list of essential medicines. This is due to regulatory barriers, a lack of awareness among healthcare providers, and weak distribution systems. To address these issues, the Indian government changed the Narcotic Drugs and Psychotropic Substances (NDPS) Act in 2014 to make it easier to get licenses for the medical use of opioids. The National Program for Palliative Care (NPPC) also focuses on making sure essential drugs are available at all levels of care. However, there are still gaps in implementation. It is important to strengthen policy enforcement, increase the skills of healthcare professionals in pain management, and improve drug supply chains. These steps are crucial to ensure that patients in need receive timely and adequate pain relief. “Policies that address essential medicines must include a list of palliative care medications. Supplies of affordable, generic medications that are “equally efficient” must be adequate and available throughout the country wherever patients live (especially opioids for pain control)”(Stjernswärd et al., 2007)
Palliative care must be strengthened by being integrated into the health system at all levels and by guaranteeing that necessary drugs, such as opioids, are available for symptom control and pain management. This entails educating the public, training medical personnel, and collaborating between primary care and specialized palliative care physicians. Palliative care must also be incorporated into national plans and goals, as well as into financial methods. India had reported some medical use of morphine for decades; it was used mainly in injection form in hospitals to relieve post-operative pain (Joranson et al., 2002).Later with the advancement of time opioid availability started increasing with the influence of various policy regulations. Access to pain-relief medications remains limited, even though the WHO includes them on its list of essential medicines. This is due to regulatory barriers, a lack of awareness among healthcare providers, and weak distribution systems. To address these issues, the Indian government changed the Narcotic Drugs and Psychotropic Substances (NDPS) Act in 2014 to make it easier to get licenses for the medical use of opioids. The National Program for Palliative Care (NPPC) also focuses on making sure essential drugs are available at all levels of care. However, there are still gaps in implementation. It is important to strengthen policy enforcement, increase the skills of healthcare professionals in pain management, and improve drug supply chains. These steps are crucial to ensure that patients in need receive timely and adequate pain relief. “Policies that address essential medicines must include a list of palliative care medications. Supplies of affordable, generic medications that are “equally efficient” must be adequate and available throughout the country wherever patients live (especially opioids for pain control)”(Stjernswärd et al., 2007)
Policy recommendation including a
comprehensive national policy for
palliative care
Palliative care should be included in the national policies and each country’s national health plans should address palliative care so that people who are living with chronic illness or at their dying stages, including children could be relieved from their sufferings to an extent. The lack of good policies can lead to unnecessary suffering and costs for patients, families, and society(Stjernswärd et al., 2007). Palliative care should be recognized as a core component of universal health coverage, integrated into primary, secondary, and tertiary care settings. National policies should coordinate palliative care with other health programs, such as those for non communicable diseases and HIV/AIDS, to leverage resources and expertise(Operational Guidelines for Palliative Care at HWC.Pdf, n.d.)India’s National Program for Palliative care(National Programme for Palliative Care (NPPC)/ :: National Health Mission, n.d.) is an example for bringing rational , quality palliative care services for people who are in need of this and also by integrating these services into the broader health care system. The programme also aims for improving the morphine availability and along with that the collaboration of national and international agencies are taken into account. The World Health Organization (WHO) recommends that all countries develop and implement palliative care policies as part of their national health strategies, emphasizing integration into primary care, community-based care, and universal health coverage schemes. The WHO’s public health model for palliative care highlights the importance of policy as a f oundational element for effective i mplementation, alongside education, medicine availability, and service delivery(Clelland et al., 2020)
Palliative care should be included in the national policies and each country’s national health plans should address palliative care so that people who are living with chronic illness or at their dying stages, including children could be relieved from their sufferings to an extent. The lack of good policies can lead to unnecessary suffering and costs for patients, families, and society(Stjernswärd et al., 2007). Palliative care should be recognized as a core component of universal health coverage, integrated into primary, secondary, and tertiary care settings. National policies should coordinate palliative care with other health programs, such as those for non communicable diseases and HIV/AIDS, to leverage resources and expertise(Operational Guidelines for Palliative Care at HWC.Pdf, n.d.)India’s National Program for Palliative care(National Programme for Palliative Care (NPPC)/ :: National Health Mission, n.d.) is an example for bringing rational , quality palliative care services for people who are in need of this and also by integrating these services into the broader health care system. The programme also aims for improving the morphine availability and along with that the collaboration of national and international agencies are taken into account. The World Health Organization (WHO) recommends that all countries develop and implement palliative care policies as part of their national health strategies, emphasizing integration into primary care, community-based care, and universal health coverage schemes. The WHO’s public health model for palliative care highlights the importance of policy as a f oundational element for effective i mplementation, alongside education, medicine availability, and service delivery(Clelland et al., 2020)
CONCLUSION
A 2019 WHO survey on non-communicable illnesses among 194 Member States found that 68% of countries had money for palliative care, whereas only 40% of countries said that at least half of patients in need received the treatments(Assessing National Capacity for t he Prevention and Control of Noncommunicable Diseases, n.d.) .Even though the need of providing palliative care is need of an hour many countries including India has to travel a lot to address the needs of the patients in need, especially in the rural settings. The emergence of palliative care movement really helps to identify how well the health system can works beyond the conventional biomedical practices. PC brings in the bio psycho social model of health and thereby helping people to relive their sufferings to great extents. So it is inevitable t o integrate palliative care into the mainstream, which includes the imparting of palliative care knowledge among the health professionals through proper trainings, sensitize the public, policy changes for making drugs available and so on. These major gaps should be addressed to make the services more effective and for the successful functioning of the palliative care system in India.
A 2019 WHO survey on non-communicable illnesses among 194 Member States found that 68% of countries had money for palliative care, whereas only 40% of countries said that at least half of patients in need received the treatments(Assessing National Capacity for t he Prevention and Control of Noncommunicable Diseases, n.d.) .Even though the need of providing palliative care is need of an hour many countries including India has to travel a lot to address the needs of the patients in need, especially in the rural settings. The emergence of palliative care movement really helps to identify how well the health system can works beyond the conventional biomedical practices. PC brings in the bio psycho social model of health and thereby helping people to relive their sufferings to great extents. So it is inevitable t o integrate palliative care into the mainstream, which includes the imparting of palliative care knowledge among the health professionals through proper trainings, sensitize the public, policy changes for making drugs available and so on. These major gaps should be addressed to make the services more effective and for the successful functioning of the palliative care system in India.
REFERENCE
Bag, S., Mohanty, S., Deep, N., Salins, N., & Bag, S. (2020). Palliative and End of Life Care in India – Current Scenario and the Way Forward. Journal of The Association of Physicians of India, 68. Bhatia, V., & Parida, S. P. (2021, May 17). (PDF) Hospice and Palliative Care: A New Movement in India. Chandra, A., Debnath, A., & Nongkynrih, B. (2023). Palliative Care Need in India: A Systematic Review and Meta-analysis. Indian Journal of Palliative Care, 29(4), 375–387. https://doi.org/10.25259/ IJPC_140_2023 Chandrasekharan Prajitha, K., Raja Subbaraman, M., Siddharth Raman, S. R., Sharahudeen, A., Chandran, D., Sawyer, J., Kumar, S., & Surendran Anish, T. (n.d.). (PDF) Need of community-based palliative care in rural India and factors that influence its sustainability: A comprehensive exploration using qualitative methodology in rural Puducherry, India. ResearchGate. Retrieved June 5, 2025. Clelland, D., van Steijn, D., Whitelaw, S., Connor, S., Centeno, C., & Clark, D. (2020). Palliative Care in Public Policy: Results from a Global Survey. Palliative Medicine Reports, 1(1), 183–190. https:/ /doi.org/10.1089/pmr.2020.0062 Devraj, V. (2022). Palliative care in India: Challenges and opportunities. The Journal of Health Design, 7, 496–499. https://doi.org/10.21853/JHD.2022.173 Ghoshal, A., Joad, A. K., Spruijt, O., Nair, S., Rajagopal, M., Patel, F., Damani, A., Deodhar, J., Goswami, D., Joshi, G., Butola, S., Singh, C., Rao, S. R., Bhatwadekar, M., Muckaden, M. A., & Bhatnagar, S. (2022). Situational analysis of the quality of palliative care services across India: A cross-sectional survey. Ecancermedicalscience, 16, 1486. https://doi.org/10.3332/ ecancer.2022.1486 Ghoshal, A., Khan Joad, A., Spruijt, O., Nair, S., Rajagopal, M., Patel, F., Damani, A., Deodhar, J., Goswami, D., Joshi, G., Butola, S., Singh, C., Rao, S. R., Bhatwadekar, M., Muckaden, M. A., & Bhatnagar, S. (2022). Situational analysis of the quality of palliative care services across India: A cross-sectional survey. Ecancermedicalscience, 16. h t t p s : / / d o i . o r g / 1 0 . 3 3 3 2 / ecancer.2022.1486 Gopal, K. S., & Archana, P. S. (n.d.). Awareness, Knowledge and Attitude about Palliative Care, in General, Population and Health Care Professionals in Tertiary Care Hospital. Jain, V. (2018). Palliative Care in India: Trials, Tribulations, and Future Prospects. Journal of Mahatma Gandhi Institute of Medical Sciences, 23(2), 55. https:// doi.org/10.4103/jmgims.jmgims_42_18 Kar, S. S., Subitha, L., & Iswarya, S. (2015). Palliative care in India: Situation assessment and future scope. Indian Journal of Cancer, 52(1), 99. https:// doi.org/10.4103/0019-509X.175578 Khosla, D., Patel, F. D., & Sharma, S. C. (2012). Palliative Care in India: Current Progress and Future Needs. Indian Journal of Palliative Care, 18(3), 149 154. https://doi.org/10.4103/0973 1075.105683 Khosla, D., Patel, F. D., & Sharma, S. C. (2012). Palliative Care in India: Current Progress and Future Needs. Indian Journal of Palliative Care, 18(3), 149–154. https://doi.org/ 10.4103/0973-1075.105683 Knaul, F. M., Bhadelia, A., Rodriguez, N. M., Arreola-Ornelas, H., & Zimmermann, C. (2018). The Lancet Commission on Palliative Care and Pain Relief— Findings, recommendations, and future directions. The Lancet Global Health, 6, S5–S6. https://doi.org/10.1016/S2214 109X(18)30082-2 Kumar, S. K. (2007). Kerala, India: A Regional Community-Based Palliative Care Model. Journal of Pain and Symptom Management, 33(5), 623–627. https:// d o i . o r g / 1 0 . 1 0 1 6 / j.jpainsymman.2007.02.005 Lijimol, A. S., Krishnan, A., Rajagopal, M. R., Gopal, B. K., & Booth, C. M. (2020). Improving Access and Quality of Palliative Care in Kerala: A Cross sectional Study of Providers in Routine Practice. Indian Journal of Palliative Care, 26(4), 500–505. https://doi.org/ 10.4103/IJPC.IJPC_17_20 Lou Kelley, M. (2007). Developing Rural Communities’ Capacity for Palliative Care: A Conceptual Model. Journal of Palliative Care, 23(3), 143–153. https:/ /doi.org/10.1177/082585970702300304 Murray, C. J., & Lopez, A. D. (1997). Mortality by cause for eight regions of the world: Global Burden of Disease Study. The Lancet, 349(9061), 1269–1276. https:/ / d o i . o r g / 1 0 . 1 0 1 6 / S 0 1 4 0 6736(96)07493-4 National Health Policy 2017 (English) .pdf. (n.d.). Retrieved June 4, 2025. National Programme for Palliative care (NPPC): National Health Mission. (n.d.). Retrieved June 27, 2025. Operational Guidelines for Palliative Care at HWC.pdf. (n.d.). Retrieved June 27, 2025. Palliative care. (n.d.). Retrieved June 2, 2025, from https://www.who.int/news-room/ fact-sheets/detail/palliative-care Rajagopal, M. (n.d.-a). THE CURRENT STATUS OF PALLIATIVE CARE IN INDIA. CANCER MANAGEMENT. Salins, N. (2020). Need for Palliative Care Education in India: Can Online Palliative Care Education Bridge These Needs? Indian Journal of Palliative Care, 26(1), 1–3. https://doi.org/10.4103/ IJPC.IJPC_7_20 Salins, N., Bhatnagar, S., Simha, S., Kumar, S., & Rajagopal, M. R. (2022). Palliative Care in India: Past, Present, and Future. Indian Journal of Surgical Oncology, 13(1), 83–90. https://doi.org/10.1007/ s13193-022-01556-0 Sepúlveda, C., Marlin, A., Yoshida, T., & Ullrich, A. (2002). Palliative Care: The World Health Organization’s global perspective. Journal of Pain and Symptom Management, 24(2), 91–96. https://doi.org/10.1016/s0885 3924(02)00440-2 Sharma, P., Thakkar, H., Patil, A., Chauhan, P., Chembon, P., AJ, S., Rana, S., Kalady, R., Wadhwani, V., Urs, G., Krishna, P., Sangma, R., Bijalwan, R., Samal, S., S, L., Naqvi, S., Bhukal, J., J, J., Rajagopal, M., & Zadey, S. (2025). Access to palliative care in India: Situational analysis and modeling of access from public healthcare centers. https:// doi.org/10.21203/rs.3.rs-6535976/v1 Stjernswärd, J., Foley, K. M., & Ferris, F. D. (2007). Integrating Palliative Care into National Policies. Journal of Pain and Symptom Management, 33(5), 514–520. h t t p s : / / d o i . o r g / 1 0 . 1 0 1 6 / j.jpainsymman.2007.02.031 Sujatha, R., & Jayagowri, K. (2017). Assessment of Palliative Care Awareness among Undergraduate Healthcare Students. Journal of Clinical and Diagnostic Research/ : JCDR, 11(9), JC06-JC10. https://doi.org/10.7860/ JCDR/2017/29070.10684 Systematic Review of Palliative Care in the Rural Setting—Marie A. Bakitas, Ronit Elk, Meka Astin, Lyn Ceronsky, Kathleen N. Clifford, J. Nicholas Dionne-Odom, Linda L. Emanuel, Regina M. Fink, Elizabeth Kvale, Sue Levkoff, Christine Ritchie, Thomas Smith, 2015. (n.d.). Retrieved June 5, 2025, from https:// journals.sagepub.com/doi/abs/10.1177/ 107327481502200411 Vijayaram, S. (1993). India: Status of cancer pain and palliative care. Journal of Pain and Symptom Management, 8(6), 421 422. https://doi.org/10.1016/0885 3924(93)90070.
Bag, S., Mohanty, S., Deep, N., Salins, N., & Bag, S. (2020). Palliative and End of Life Care in India – Current Scenario and the Way Forward. Journal of The Association of Physicians of India, 68. Bhatia, V., & Parida, S. P. (2021, May 17). (PDF) Hospice and Palliative Care: A New Movement in India. Chandra, A., Debnath, A., & Nongkynrih, B. (2023). Palliative Care Need in India: A Systematic Review and Meta-analysis. Indian Journal of Palliative Care, 29(4), 375–387. https://doi.org/10.25259/ IJPC_140_2023 Chandrasekharan Prajitha, K., Raja Subbaraman, M., Siddharth Raman, S. R., Sharahudeen, A., Chandran, D., Sawyer, J., Kumar, S., & Surendran Anish, T. (n.d.). (PDF) Need of community-based palliative care in rural India and factors that influence its sustainability: A comprehensive exploration using qualitative methodology in rural Puducherry, India. ResearchGate. Retrieved June 5, 2025. Clelland, D., van Steijn, D., Whitelaw, S., Connor, S., Centeno, C., & Clark, D. (2020). Palliative Care in Public Policy: Results from a Global Survey. Palliative Medicine Reports, 1(1), 183–190. https:/ /doi.org/10.1089/pmr.2020.0062 Devraj, V. (2022). Palliative care in India: Challenges and opportunities. The Journal of Health Design, 7, 496–499. https://doi.org/10.21853/JHD.2022.173 Ghoshal, A., Joad, A. K., Spruijt, O., Nair, S., Rajagopal, M., Patel, F., Damani, A., Deodhar, J., Goswami, D., Joshi, G., Butola, S., Singh, C., Rao, S. R., Bhatwadekar, M., Muckaden, M. A., & Bhatnagar, S. (2022). Situational analysis of the quality of palliative care services across India: A cross-sectional survey. Ecancermedicalscience, 16, 1486. https://doi.org/10.3332/ ecancer.2022.1486 Ghoshal, A., Khan Joad, A., Spruijt, O., Nair, S., Rajagopal, M., Patel, F., Damani, A., Deodhar, J., Goswami, D., Joshi, G., Butola, S., Singh, C., Rao, S. R., Bhatwadekar, M., Muckaden, M. A., & Bhatnagar, S. (2022). Situational analysis of the quality of palliative care services across India: A cross-sectional survey. Ecancermedicalscience, 16. h t t p s : / / d o i . o r g / 1 0 . 3 3 3 2 / ecancer.2022.1486 Gopal, K. S., & Archana, P. S. (n.d.). Awareness, Knowledge and Attitude about Palliative Care, in General, Population and Health Care Professionals in Tertiary Care Hospital. Jain, V. (2018). Palliative Care in India: Trials, Tribulations, and Future Prospects. Journal of Mahatma Gandhi Institute of Medical Sciences, 23(2), 55. https:// doi.org/10.4103/jmgims.jmgims_42_18 Kar, S. S., Subitha, L., & Iswarya, S. (2015). Palliative care in India: Situation assessment and future scope. Indian Journal of Cancer, 52(1), 99. https:// doi.org/10.4103/0019-509X.175578 Khosla, D., Patel, F. D., & Sharma, S. C. (2012). Palliative Care in India: Current Progress and Future Needs. Indian Journal of Palliative Care, 18(3), 149 154. https://doi.org/10.4103/0973 1075.105683 Khosla, D., Patel, F. D., & Sharma, S. C. (2012). Palliative Care in India: Current Progress and Future Needs. Indian Journal of Palliative Care, 18(3), 149–154. https://doi.org/ 10.4103/0973-1075.105683 Knaul, F. M., Bhadelia, A., Rodriguez, N. M., Arreola-Ornelas, H., & Zimmermann, C. (2018). The Lancet Commission on Palliative Care and Pain Relief— Findings, recommendations, and future directions. The Lancet Global Health, 6, S5–S6. https://doi.org/10.1016/S2214 109X(18)30082-2 Kumar, S. K. (2007). Kerala, India: A Regional Community-Based Palliative Care Model. Journal of Pain and Symptom Management, 33(5), 623–627. https:// d o i . o r g / 1 0 . 1 0 1 6 / j.jpainsymman.2007.02.005 Lijimol, A. S., Krishnan, A., Rajagopal, M. R., Gopal, B. K., & Booth, C. M. (2020). Improving Access and Quality of Palliative Care in Kerala: A Cross sectional Study of Providers in Routine Practice. Indian Journal of Palliative Care, 26(4), 500–505. https://doi.org/ 10.4103/IJPC.IJPC_17_20 Lou Kelley, M. (2007). Developing Rural Communities’ Capacity for Palliative Care: A Conceptual Model. Journal of Palliative Care, 23(3), 143–153. https:/ /doi.org/10.1177/082585970702300304 Murray, C. J., & Lopez, A. D. (1997). Mortality by cause for eight regions of the world: Global Burden of Disease Study. The Lancet, 349(9061), 1269–1276. https:/ / d o i . o r g / 1 0 . 1 0 1 6 / S 0 1 4 0 6736(96)07493-4 National Health Policy 2017 (English) .pdf. (n.d.). Retrieved June 4, 2025. National Programme for Palliative care (NPPC): National Health Mission. (n.d.). Retrieved June 27, 2025. Operational Guidelines for Palliative Care at HWC.pdf. (n.d.). Retrieved June 27, 2025. Palliative care. (n.d.). Retrieved June 2, 2025, from https://www.who.int/news-room/ fact-sheets/detail/palliative-care Rajagopal, M. (n.d.-a). THE CURRENT STATUS OF PALLIATIVE CARE IN INDIA. CANCER MANAGEMENT. Salins, N. (2020). Need for Palliative Care Education in India: Can Online Palliative Care Education Bridge These Needs? Indian Journal of Palliative Care, 26(1), 1–3. https://doi.org/10.4103/ IJPC.IJPC_7_20 Salins, N., Bhatnagar, S., Simha, S., Kumar, S., & Rajagopal, M. R. (2022). Palliative Care in India: Past, Present, and Future. Indian Journal of Surgical Oncology, 13(1), 83–90. https://doi.org/10.1007/ s13193-022-01556-0 Sepúlveda, C., Marlin, A., Yoshida, T., & Ullrich, A. (2002). Palliative Care: The World Health Organization’s global perspective. Journal of Pain and Symptom Management, 24(2), 91–96. https://doi.org/10.1016/s0885 3924(02)00440-2 Sharma, P., Thakkar, H., Patil, A., Chauhan, P., Chembon, P., AJ, S., Rana, S., Kalady, R., Wadhwani, V., Urs, G., Krishna, P., Sangma, R., Bijalwan, R., Samal, S., S, L., Naqvi, S., Bhukal, J., J, J., Rajagopal, M., & Zadey, S. (2025). Access to palliative care in India: Situational analysis and modeling of access from public healthcare centers. https:// doi.org/10.21203/rs.3.rs-6535976/v1 Stjernswärd, J., Foley, K. M., & Ferris, F. D. (2007). Integrating Palliative Care into National Policies. Journal of Pain and Symptom Management, 33(5), 514–520. h t t p s : / / d o i . o r g / 1 0 . 1 0 1 6 / j.jpainsymman.2007.02.031 Sujatha, R., & Jayagowri, K. (2017). Assessment of Palliative Care Awareness among Undergraduate Healthcare Students. Journal of Clinical and Diagnostic Research/ : JCDR, 11(9), JC06-JC10. https://doi.org/10.7860/ JCDR/2017/29070.10684 Systematic Review of Palliative Care in the Rural Setting—Marie A. Bakitas, Ronit Elk, Meka Astin, Lyn Ceronsky, Kathleen N. Clifford, J. Nicholas Dionne-Odom, Linda L. Emanuel, Regina M. Fink, Elizabeth Kvale, Sue Levkoff, Christine Ritchie, Thomas Smith, 2015. (n.d.). Retrieved June 5, 2025, from https:// journals.sagepub.com/doi/abs/10.1177/ 107327481502200411 Vijayaram, S. (1993). India: Status of cancer pain and palliative care. Journal of Pain and Symptom Management, 8(6), 421 422. https://doi.org/10.1016/0885 3924(93)90070.
Conflict of interest: None
Role of funding source: None
