
Indian Journal of Health Social Work
(UGC CARE List Journal)
EARLY ONSET OF SCHIZOPHRENIA: A CASE STUDY OF HIGH GENETIC LOADING IN THE FAMILY OF ORIGIN AND PROCREATION
Neinunnem Grace Khaute1, Virupaksha Kiccha2, Gobinda Majhi3
1State Project Coordinator, NIMHANS- UNDP, Department of Psychiatric Social Work, National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru-29, Karnataka, India, 2PhD Scholar, Department of Psychiatric Social Work, National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru-29, Karnataka, India, 3Associate Professor, Department of Psychiatric Social Work, National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru-29, Karnataka, India
Correspondence: Gobinda Majhi, e-mail: majhi.gobinda10@gmail.com
ABSTRACT Family plays a very important role in the promotion of one’s mental wellbeing. Often times, it is found that individual with a high family psychopathology are more at risk of developing mental illness Early exposure to a disturbed environment during childhood can have a psychological impact in the individual which further can also affect the marital life. This is a typical case of the impact of high genetic loading in the family of origin which was further carried to the family of procreation. Key words: family of origin, family of procreation, genetic loading. INTRODUCTION Early onset of schizophrenia can have a persistent adverse effect on an individual’s physical and mental health wellbeing. It is also believed to be associated with decreased functionality due to multiple relapses and hospitalization which hampers one to function fully especially when it comes to establishing the family of procreation. It is found that multiple relapses often occur after marriage. Studies have shown that the success rates of ma r r i age a re lower in patients with s chizophrenia. Several factor s include multiple relapses due to marital stress, marriage acting as both the risk and maintain factor of the illness, sexual dissatisfaction, stigma and misconception etc. (Srivastava, 2013). This case is about a patient with an early onset of schizophrenia with a high genetic loading in the family of origin. Case report: Mrs. Y is a 22-year-old married female, born in a Hindu family, studied upto 8th standard, belonging to a lower socio- economic status hailing from Anekal, Bangalore. Patient was diagnosed of schizophrenia since the past 15 years with insidious in onset and continuous with episodic exacerbation in course along with a history of multiple seizures in the past, history of attempted suicide in mother, marital discord in parents and patient herself, history of mental retardation in brother with history of cannabis used in father and poor social support both primary and secondary, poor knowledge regarding the illness of the patient from the family of origin and procreation Patient had an arranged marriage on 2016. The families of procreation were not informed about her illness. Few days later after her wedding, she was abused by her husband and in-laws both verbally and physically due to her decreased functionality coupled with dowry related issue. Patient was reported to have multiple burnt marks and injuries where the patient’s mother lodged a complaint against the in-laws at Sarjapura’s Police Station. However, a settlement was done between the two parties after several negotiations. As part of the negotiation patient’s family were given some amount of money as compensation. From the time patient got married, she was off medication where her symptoms relapsed following the incident and was brought to Shor t St ay Wa rd on compl aint s of unresponsiveness and was advised inpatient care. Since then, patient was taken to her mother’s place. Subsequent to that patient was again brought to NIMHANS on complaints of multiple body pains, muttering and laughing to self, expressing sadness and crying spells, expressing death wishes, withdrawn behavior, disturbed sleep, appetite and self -care.Reasons for referral:
The case was referred to the psychiatric social work team for Psychosocial assessment and Intervention.
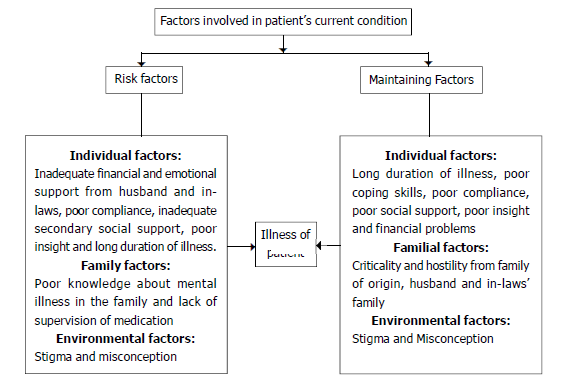
Diagrammatic Representation of Psychosocial Analysis and Diagnosis
Objectives of Intervention
1. To improve the level of insight towards illness
2. To enhance drug and t reatment compliance
3. To help engage in regular follow-up to maintain medication adherence.
4. To reduce stigma and misconception
5. To reduce expressed emotion The intervention was provided at two
levels, one at the individual level and the other at the family level.
Psychoeducation:
A therapeutic relationship was established and psychoeducation was provided as part of the intervention. The sessions were focused on providing information about the nature of the illness, its relation with stressors in the patient’s life and her ways of coping, identifying early signs of relapse and the factors associated with, the stress – vulnerability model and the steps patient can take to maintain her mental health, like engaging in meaningful activities and regular follow up for treatment.
Addressing expressed emotion:
Five minutes speech sample was taken from the mother. Patient’s mother was found to be critical towards patient. It was found that mother would displace her anger towards the patient by scolding and shouting at her. The mother was made to understand the negative impact which could have on the patient due to high expressed emotions.
Addressing stigma and misconception:
Family members of a patient with mental illness usually faced stigma and have misconception about mental illness. As a result, parents tend to blame themselves for their children’s illness or either becomes critical and hostile to them. Often patients are taken for medico- religious practices where family members spend an enormous amount of money but to no avail. In other cases, the patients are secluded from the society. Family members often believe that mental illness is due to some magic or a punishment from god. Such misconceptions were cleared.
Arranging for free medication:
A request letter for free medication was given to the Resident Medical Officer which as approved. Patient was provided with free medication after the approval.
Pre discharge counseling:
Pre-discharge counseling was given to the patient and mother. The importance of regular medication, practicing a healthy lifestyle and engaging in small household chores so as to maintain the functionality of the patient were discussed. Importance of regular follow- ups and monitoring of medication was discussed which was conducted over two sessions.
OUTCOME
1. Insight facilitation was provided.
2. Family member developed knowledge regarding mental illness.
3. Expressed emotion was reduced to some extend from the mother
4. Welfare benefits were received.
DISCUSSION
Ms. Y is a 22-year-old married woman, born from a non- consanguineous marriage, studied upto the 8th std. She was temperamentally, a slow to warmth child, with a family history of marital discord in the parents where father deserted the family 20 years ago leaving the family with no economic support. The personal history of the patient revealed early onset of illness, with many breakthrough episodes and multiple relapses secondary to poor drug compliance due to poor insight, inadequate supervision of medication and inadequate social support. The family history showed marital discord in parents and patient herself with substance use in the father and mental retardation in brother along with expressed emotions in the form of criticality and hostility from the family procreation and partly from the family of origin. The patient has an illness of more than 15 years. In a study by (Matheson et al., 2017) showed the childhood maltreatment and history of parental schizophrenia spectrum disorders were associated with the early onset of schizophrenia. Some studies have shown that childhood trauma may be associated with one’s mental health and wellbeing. Childhood trauma maybe in the forms of bullying, victimization, parental loss and separation, abuse, negligence in terms of physical and emotional negligence (Norman et al., 2012; Varese et al ., 2012). In this case, the psychosocial analysis revealed multiple risk and maintaining factors to the patient’s illness. The patient has many breakthrough episodes and multiple relapses secondary to poor drug compliance due to poor insight, inadequate supervision of medication and inadequate social support. A study conducted in Pakistan showed that the prime factors concomitant to multiple relapses were treatment nonadherence due to poor insight fear of the patient, poor socio- economic status of the patient and possible side effects (Ahmad etal., 2017). It is a known fact that nonadherence is commonly seen among patients with schizophrenia mostly due significant psychopathology, stigma related issues and various cultural factors. Non- adherence among patients wi th mental i llness has become a serious problem as there are mul t iple relapses leading to f requent hospitalization due to the exacerbation of symptoms and declined in their functionality (Phan, 2016).
Family plays a very important role in the prevention of relapses of individuals with schizophrenia. Significant expressed emotion in the form of criticality, hostility and over involvement leads to multiple relapses and hospitalization compared to families with less express emotion. Addressing the expressed emotions of the family at all levels have been widel y use d a s par t of psychosocial intervention (Pharoah et al., 2010). Patient’s mother was psycho-educated about the illness of the patient which focused on imparting statement of diagnosi s, earl y warning symptoms, importance of medication and continued treatment and relapse prevention. It was also on reducing critical comments towards the patient and an appropriate way of communicating with the patient, without being indifferent, but at the same time, fostering the patient’s independence. High expressed emotions and how genetic loading can be a causal factor for schizophrenia as wel l as mul tiple relapses were fur ther addressed. There have been recent studies on the direct and indirect effects of offspring of couples with mental health problems. It is said that intrauterine environment, antenatal and postnatal exposure to depression have a high risk on the offspring. Some of the indirect impacts found were poor economic condition, marital discord in parents along with dysfunctional pattern of communication in the family and various other psychosocial stressors during childhood (Alvus et al., 1994; Tsuang, 2000; Manning et al., 2006). Various studies have shown that the factors of multiple relapses include substance abuse, forgetfulness, anxiety about side effect, inadequate knowledge, lack of insight, lack of motivation fear of stigma, poor patient health care provider relationship, poor services and acces s to servi ces and low economi c conditions (Lacro et al., 2002; Fenton et al., 1997). Stressful life events such as depression were also found to be associated wi th relapses (Siris, 2000). Adherence to treatment was also found to be poor in case of poor insight and discontinuation of medication prematurely (Hunter et al., 1994). In India, there has always been a misconception that marriage would solve almost all problems even mental disorders (Behere et al., 2011). As a result, the prevalence of marriage of individuals with mental disorders before the marriage is quite common in India. However, various studies have found that patients with schizophrenia develop more stress after marriage and reports of higher undesirable events post marriage. Around the globe, violence against women has become a major health concern both in the society and family whi ch includes wome n wi th chroni c schizophrenia. Studies have found that women with severe mental illness are 2- 8 times more likely to be victims of sexual and domestic violence compared to the general population (K hal i fe h et al ., 2 015 ) . Women wi th schizophrenia are more at risk of intimate partner violence that are more in the form verbal and physical assault associated with psychopathology (Afe et al., 2016). Higher marital discords and abuses have also been found among patients with mental illness (Dominian, 1979: Das et al., 1997).
This case shows that the early exposure to childhood trauma can highly have an impact in an individual’s mental health problems such as depression, anxiety and stress with early psychosis. Literatures have also shown that childhood trauma is commonly associated with an early onset of exhibi ting psychot ic symptoms (Ramsay et al., 2011; Wang et al., 2011; Bendal et al., 2013). Bearing this in mind, it is important to address the early psychosis treatment program for patients who have experienced childhood trauma. However, at times most treating teams are reluctant to enquire about such cases on fear of rupture of rapport between the patient and the treating team. Understanding the patient’s childhood trauma as well as the trauma which the patient faced later in life needs to be taken into account for an effective intervention. Further, psychiatric social work intervention requi res a detai led assessment of the ps ychosocia l i s sues prevai l ing at the individual, familial and community level. Understanding the underlying problems of such issues will help in framing and providing a better intervention plan.
REFERENCES
Afe, T. O., Emedoh, T. C., Ogunsemi, O., & Adegbohun, A. A. (2016). Intimate partner violence, psychopathology and the women with schizophrenia in an outpa t ie nt cl i ni c Sout h-Sout h, Nigeria. BMC psychiatry, 16(1), 197.
Ahmad, I., Khalily, M. T., & Hallahan, B. (2017). Reasons associated with treatment non-adherence in schizophrenia in a Pakistan cohort. Asian journal of psychiatry, 30, 39-43.
Al bus , M., Scher er, J ., Hue ber, S., Lechleuthner, T., Kraus, G., Zausinger, S., & Burkes, S. (1994). The impact of fami l ia l l oading on gender di f fe rences in a ge at ons et of schizophrenia. Acta Psychiat ri ca Scandinavica, 89(2), 132-134.
Behere, P. B., Rao, S. T., & Verma, K. (2011). Effect of marriage on pre-existing ps ycho ses . Indi an jo ur na l of psychiatry, 53(4), 287.
Bendall, S., Hulbert, C. A., Alvarez-Jimenez, M., Al lott, K., McGorry, P. D., & Jackson, H. J. (2013). Testing a model of the relationship between childhood sexual abuse and psychosis in a firstepisode psychosis group: the role of ha l lucinat ions a nd del us ions , posttraumatic intrusions, and selective attention. The Journal of nervous and mental disease, 201(11), 941-947.
Das, M. K., Kulhara, P. L., & Verma, S. K. (1997). Life events preceding relapse of s chizophrenia. I nternat ional Journal of Social Psychiatry , 43 (1), 56-63.
Dominian, J. (1979). Marriage and psychiatric il lness. British medical journal , 2 (6194), 854.
Fenton, W. S., Blyler, C. R., & Heinssen, R. K. (1997). Determinants of medication compliance in schizophrenia: empirical and clinical findings. Schizophrenia bulletin, 23 (4), 637-651.
Hunter E. P., & Storat, B. (1994). Psychosocial triggers of relapse in persons with chroni c me nta l i l l nes s : A pi l ot s t udy. I s sues in me nt al he al th nursing, 15 (1), 67-72.
Khalifeh, H., Moran, P., Borschmann, R., Dean, K., Hart, C., Hogg, J., … & Howard, L. M. (2015). Domestic and sexual violence against patients with severe me nta l i l l nes s . Ps ycholo gi c al medicine, 45 (4), 875-886.
Lacro, J .P., Dunn, L. B., Dolder, C. R., Leckband, S. G., & Jeste, D. V. (2002). Prevalence of and risk factors for medication non adherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry, 63(10), 892- 909.
Manning, C., & Gregoire, A. (2006). Effects of pa renta l ment al i l l ne s s on children. Psychiatry , 5(1), 10-12.
Matheson, S. L., Kariuki, M., Green, M. J., Dean, K., Harris, F., Tzoumakis, S., … & Car r, V. J . (2017) . Effects of ma l t r eatment a nd par ent al schizophrenia spectrum disorders on early chi ldhood social -emotional functioning: a population record l inkage study. Epidemiology and psychiatric sciences , 26(6), 612-623.
Norman, R. E., Byambaa, M., De, R., Butchart, A., Scott, J., & Vos, T. (2012). The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS medicine, 9(11), e1001349.
Phan, S. V. (2016). Medication adherence in patients wi th schizophrenia. The International Journal of Psychiatry in Medicine, 51(2), 211-219.
Pharoah, F., Mari, J. J., Rathbone, J., & Wong, W. (2010). Family intervention for schizophrenia. Cochrane database of systematic reviews , (12).
Ramsay, C. E., Flanagan, P., Gantt, S., Broussard, B., & Compton, M. T. (2 011 ) . Cl i ni c al co r re lat es of ma l t r ea tme nt and t r aumat i c ex per ie nce s i n chi ldhoo d a nd adolescence among predominantly Af r i c an Amer i can, s oc ial l y disadvantaged, hospitalized, firstepisode psychosis patients. Psychiatry research, 188(3), 343-349.
Si r i s , S. G. ( 200 0) . De pre s s i on in schizophrenia: perspective in the era of “ aty pi c al ” a nt ips ychot i c agent s . Amer i ca n J ourna l of Psychiatry, 157(9), 1379-1389.
Sr i vas tav a, A. (2013) . Mar r iage a s a perceived panacea to mental illness in India: Reality check. Indian journal of psychiatry, 55(Suppl 2), S239.
Tsuang, M. (2000). Schizophrenia: genes and e n v i r o n m e n t . B i o l o g i c a l psychiatry, 47(3), 210-220.
Varese, F., Smeets, F., Drukker, M., Lieverse, R., Lataster, T., Viechtbauer, W., … & Bental l , R. P. (2012). Chi ldhood adver s i t ies increase the r i sk of psychosis: a meta-analysis of patientcont rol , prospect i ve-and cros s – se ct ional co ho r t studies. Schizophrenia bulletin, 38(4), 661-671.
Wang, Z., Xue, Z., Pu, W., Yang, B., Li, L., Yi, W., … & Rosenheck, R. A. (2013). Comparison of fi rst episode and chronic patients diagnosed wi th s chi zophre ni a: s ympt oms a nd childhood trauma. Early intervention in psychiatry, 7(1), 23-30.
Conflict of interest: None
Role of funding source: None
It’s a matter of great pride for me that All India Association of Medical Social Work Professionals is launching first issue of “Indian Journal of Health Social Work” on the auspicious occasion of 6th Annual National Conference of AIAMSWP, 2019.
Actually no matter if someone doesn’t know afterward its up to other users that they will assist, so here it happens.
Wow, that’s what I was seeking for, what a information! present here at this webpage, thanks admin of this web site.
Excellent blog! Do you have any tips and hints for aspiring writers? I’m planning to start my own site soon but I’m a little lost on everything. Would you recommend starting with a free platform like WordPress or go for a paid option? There are so many choices out there that I’m totally confused .. Any suggestions? Cheers!
What’s up, just wanted to tell you, I loved this post. It was practical. Keep on posting!
Unquestionably imagine that that you said. Your favorite reason seemed to be at the internet the easiest factor to take into account of. I say to you, I definitely get annoyed while folks consider concerns that they plainly do not recognize about. You controlled to hit the nail upon the top as neatly as defined out the whole thing with no need side effect , people could take a signal. Will probably be back to get more. Thank you
This post is in fact a nice one it assists new the web people, who are wishing in favor of blogging.
Hi! Do you know if they make any plugins to safeguard against hackers? I’m kinda paranoid about losing everything I’ve worked hard on. Any recommendations?
I am sure this paragraph has touched all the internet visitors, its really really fastidious piece of writing on building up new webpage.
Hi i am kavin, its my first time to commenting anyplace, when i read this post i thought i could also make comment due to this sensible article.
I like the valuable information you provide in your articles. I’ll bookmark your weblog and check again here frequently. I am quite certain I will learn plenty of new stuff right here! Good luck for the next!
Simply want to say your article is as amazing. The clarity in your post is simply nice and i can assume you are an expert on this subject. Well with your permission let me to grab your RSS feed to keep up to date with forthcoming post. Thanks a million and please keep up the enjoyable work.
Hi, I would like to subscribe for this weblog to take hottest updates, thus where can i do it please help.
If you are going for best contents like I do, only visit this site everyday as it presents quality contents, thanks
WOW just what I was looking for. Came here by searching for %meta_keyword%
Everything is very open with a very clear explanation of the issues. It was really informative. Your site is useful. Many thanks for sharing!
Really when someone doesn’t know then its up to other people that they will assist, so here it happens.
Quality articles is the crucial to attract the users to pay a quick visit the website, that’s what this site is providing.
Appreciating the dedication you put into your blog and in depth information you provide. It’s nice to come across a blog every once in a while that isn’t the same old rehashed information. Fantastic read! I’ve bookmarked your site and I’m including your RSS feeds to my Google account.
My brother suggested I might like this blog. He was once entirely right. This publish actually made my day. You cann’t consider just how a lot time I had spent for this info! Thanks!
Wow that was strange. I just wrote an really long comment but after I clicked submit my comment didn’t show up. Grrrr… well I’m not writing all that over again. Anyhow, just wanted to say wonderful blog!
Woah! I’m really enjoying the template/theme of this site. It’s simple, yet effective. A lot of times it’s very hard to get that “perfect balance” between user friendliness and visual appearance. I must say you have done a awesome job with this. Also, the blog loads super fast for me on Firefox. Outstanding Blog!
Do you mind if I quote a couple of your articles as long as I provide credit and sources back to your site? My blog site is in the exact same area of interest as yours and my visitors would really benefit from some of the information you present here. Please let me know if this ok with you. Regards!
If some one wants to be updated with most recent technologies afterward he must be pay a visit this website and be up to date daily.
Amazing! Its really awesome article, I have got much clear idea concerning from this post.
I don’t know if it’s just me or if perhaps everybody else experiencing problems with your site. It appears like some of the written text in your posts are running off the screen. Can somebody else please provide feedback and let me know if this is happening to them as well? This might be a issue with my internet browser because I’ve had this happen before. Cheers
Write more, thats all I have to say. Literally, it seems as though you relied on the video to make your point. You clearly know what youre talking about, why waste your intelligence on just posting videos to your weblog when you could be giving us something informative to read?
I think everything published made a bunch of sense. However, think about this, suppose you typed a catchier post title? I ain’t suggesting your information is not good., but what if you added a post title to possibly get a person’s attention? I mean EARLY ONSET OF SCHIZOPHRENIA: A CASE STUDY OF HIGH GENETIC LOADING IN THE FAMILY OF ORIGIN AND PROCREATION is a little vanilla. You should glance at Yahoo’s front page and see how they create post headlines to grab viewers to click. You might add a video or a picture or two to get people excited about everything’ve got to say. In my opinion, it would bring your posts a little bit more interesting.
Usually I do not read post on blogs, but I wish to say that this write-up very forced me to take a look at and do it! Your writing taste has been amazed me. Thanks, very great post.
This is my first time pay a quick visit at here and i am truly pleassant to read all at single place.
This is very interesting, You’re a very skilled blogger. I have joined your feed and look forward to seeking more of your magnificent post. Also, I’ve shared your site in my social networks!
It’s amazing to visit this web page and reading the views of all colleagues regarding this paragraph, while I am also keen of getting experience.
Hi there would you mind letting me know which webhost you’re using? I’ve loaded your blog in 3 completely different browsers and I must say this blog loads a lot faster then most. Can you suggest a good internet hosting provider at a fair price? Cheers, I appreciate it!
Does your website have a contact page? I’m having a tough time locating it but, I’d like to send you an e-mail. I’ve got some creative ideas for your blog you might be interested in hearing. Either way, great blog and I look forward to seeing it grow over time.