Background: Menstruation is considered a universal experience, but transition-aged youth in
tribal communities often remain critically underinformed about menstrual hygiene. The pervasive
influence of cultural taboos and misinformation, coupled with inadequate access to essential
facilities and sanitary products, exacerbates health risks and emotional distress. Aim: This study
aimed to explore menstrual knowledge, attitudes, and practices among transitioned-aged young
women in the Siddi tribe. Methods and Materials: The study employed an exploratory design
with purposive sampling of 32 participants from the Siddi tribal community in Yellapur Taluka,
Karnataka. Data were collected through semi-structured interviews and analyzed thematically to
uncover key themes. Results: Thematic analysis yielded four principal themes: access to
menstrual hygiene products, hygiene practices, privacy and facilitation, stigma and myths, health
and wellbeing, and menstrual knowledge and awareness. Within these overarching themes, several
sub-themes were accentuated, supported by direct verbatims from the interviews, providing
nuanced insights into the participants’ experiences. Conclusion: The study revealed low
menstruation-related knowledge among Siddi tribal women, with menarche typically starting at
age 14. Early marriage is common, with 62.5% of transitioned-aged women already married,
contrasting with other tribes where marriage often occurs later. Many women have poor
understanding of menstruation, relying on misinformation from friends and family, which contributes to health issues. Menstruation remains taboo, influenced by cultural and religious
factors, with common rituals and inadequate hygiene practices. Many women use reusable clothes
under poor conditions, raising health risks. These findings emphasize the need for targeted
interventions to enhance menstrual health education, accessibility, and cultural sensitivity within
the Siddi community, fostering improved psychological well-being.
Transition-aged youth (15-29 years) confront
several transitional challenges (Dar &
Sobhana, 2024). This transitional period is
marked by menarche, a significant milestone
often surrounded by traditions, myths, and
misconceptions within Indian culture.
Menstruation is a fundamental aspect of a
woman’s life, perceived differently across
various social and cultural landscapes.
Despite being a routine biological function, it
continues to be cloaked in stigma, taboos, and
secrecy (Mudi et al., 2023). Pervasive myths,
such as the prohibition of entering religious
spaces, designate women as impure, leading
to their exclusion from worship and imposition
of various domestic restrictions, including
cooking and handling certain foods. These
taboos, seldom confronted in public or private
discourse, foster misconceptions and
insufficient menstrual preparedness. The
consequent psychological distress and societal
constraints on daily life are acutely observed
in rural and tribal areas, notwithstanding
gradual changes among urban, educated
populations (Upashe et al., 2015). The
insufficient management of menstrual hygiene
(MHM) is a global issue, particularly in low
and middle-income countries, where
individuals frequently lack the requisite
knowledge, confidence, and skills to manage
their menstrual health effectively. (Garg &
Anand, 2015). Maintaining MHM is vital for the
health and dignity of menstruating women.
Effective MHM requires access to basic
amenities, including clean absorbent
materials, water, soap, and private sanitation
facilities. The selection and proper use of
menstrual absorbents are crucial, as
inadequate MHM can lead to serious health
issues, such as genital and urinary tract
i nfections. As per the World Health
Organization (WHO), 1.7 billion people
globally lack access to basic sanitation,
compelling many women to resort to
unsanitary materials due to insufficient
awareness and the high cost of menstrual
products. (WHO, 2023). A study carried out
in Odisha found a strong association between
the increased occurrence of reproductive tract
infections (RTIs) and poor menstrual hygiene,
emphasizing the broader health and economic
consequences. (Torondel et al., 2018). Open
communication about menstrual hygiene
management (MHM) is vital, as inadequate
MHM hinders the progress of several
Sustainable Development Goals (SDGs),
particularly those related to gender equality,
education, and economic participation.
Understanding and improving MHM is essential
not only for individual well-being but also for
t he advancement of broader societal
objectives. Despite its significance, menstrual
hygiene remains a neglected issue, requiring
greater attention and action to ensure
women’s health, empowerment, and overall
societal progress.
In India, social group affiliation critically
i nfluences access to resources, with
marginalised groups such as Scheduled
Castes (SC) and Scheduled Tribes (ST) consistently lagging in socioeconomic
development and health outcomes (Ram et al.,
2020). These communities often lack essential
information on safeguarding women’s health
during
menstruation, leading to
disproportionate susceptibility to preventable
reproductive health issues and limited
knowledge of hygienic practices. Research in
Odisha’s tribal districts found that over one
third of adolescent girls use unsanitary
materials as menstrual absorbents, with cloth
remaining a preferred choice due to its
availability and low cost (Mishra, 2020).
Significant disparities in menstrual hygiene
practices are apparent, as indicated by the
National Family Health Survey (2019–21),
which shows that 59% of tribal women aged
15–24 use cloth, compared to just 25% of
women from the general castes (Ram et al.,
2020).
A recent analysis of nationally representative
survey data on menstrual hygiene
management in India reveals troubling trends.
Fewer than 40% of transitioned-aged (15
24years) women use disposable absorbents
exclusively, with most relying on reusable
materials such as clothes, which can increase
health risks (Ram et al., 2020). The study
reveals significant disparities driven by
personal, family, and community factors. In
rural and non-southern regions of India, as
well as among women with lower
socioeconomic status, less education, and
those from tribal and minority communities,
the use of disposable absorbents is notably
infrequent.
The higher use of disposable absorbents in
southern states is attributed to better
resources, infrastructure, and higher female
literacy. For example, Tamil Nadu schools
provide separate toilet and menstrual waste
disposal facilities, unlike those in Maharashtra
and Chhattisgarh (Sivakami et al., 2019).
Rural women have less menstrual hygiene
knowledge compared to their urban peers,
impacting their practices. Findings of the study
revealed that there is more frequent
commercial pad usage in urban areas and
continued reliance on clothes in rural and
tribal regions.
Ram et al., in 2020, reported a particularly
low rate of exclusive disposable absorbent use
among young women from Scheduled Tribes,
with less than a quarter using them compared
to nearly half from general castes. Caste
identity remains a significant factor in social
inclusion and access to resources. Despite
policies aimed at improving conditions for
lower-caste individuals, the study emphasizes
the need to prioritise menstrual hygiene within
these efforts. Kumar and his associate have
identified a substantial gap in menstrual
knowledge and management among tribal
women, influenced by access, financial
constraints, and cultural practices (Kumar &
Srivastava, 2011).
This primary objective was to explore the
cultural context of menstruation in the Siddi
tribal community and address cultural nuances
and unique challenges to develop culturally
i nformed interventions and education
initiatives that enhance menstrual hygiene and
community well-being. The study underscores
the crucial role of education, economic status,
and regional influences in shaping menstrual
hygiene practices.
Data for this qualitative study were collected
through interviews and analyzed thematically.
The iterative theme analysis method—
comprising grouping, coding, identifying,
assessing, defining, and reporting themes and
sub-themes—transformed unstructured data
into meaningful insights (Clarke & Braun,
2017). This approach allowed for the
extraction of significant themes by identifying
patterns within the data. Purposeful sampling selected a total of 32 participants, as detailed
in Table 1. The limited sample size can be
attributed to the isolated nature of the tribal
community, where each participant lived
approximately ten kilometers apart in the
forest.
Eligibility for participation required
membership in the Siddi tribal community,
willingness to participate, and effective
communication skills. Participants were
provided with comprehensive information
about the study before the interviews, and
mutually convenient times were arranged.
Additionally, demographic data, including age,
gender, and religion, were collected from the
participants. This study was conducted with
t ransitional-aged women residing in
underprivileged areas of Yellapur Taluk,
Karwar district, Karnataka, India, from
October 28 to November 6, 2023. It was part
of the curriculum for the Honour’s Bachelor’s
program in Public Health and Masters Social
Work at the Karnataka State Rural
Development and Panchayat Raj University.
The Social Work Department organized a ten
day Tribal Camp (RDPRU/02/PHSW/2021) as
part of the curriculum, which provided insights
into the health, customs, and culture of the
Siddi tribal community, with a particular
emphasis on menstrual hygiene. Data
collection was collected by four female
researchers, with each interview lasting a
minimum of one hour and thirty minutes. A
total of 32 participants were selected through
purposive sampling. The right to privacy for
participants was rigorously maintained
throughout the study. Interviews were
conducted in confidential settings without the
presence of any additional individuals.
Participation was entirely voluntary, with
minimal risks involved, and all information
shared was ensured to be kept confidential
by providing participatory information (PI)
forms and consent information sheets (CIS)
detailing ethical considerations, including
informed consent, confidentiality, and privacy,
given the sensitive nature of the topic. These
measures ensured that participants
understood their rights and the protections for
their personal information.
Prior to data collection, the researchers
undertook an extensive review of menstrual
hygiene practices among tribal communities,
with a specific focus on the Siddi tribe due to
their comparatively low educational status.
The four researchers were trained for data
collection procedures, including the
administration of semi-structured interviews
prior to data collection. The right to privacy
for participants was rigorously maintained
throughout the study. Interviews were
conducted in confidential settings without the
presence of any additional individuals.
Participants were given consent forms and
information sheets detailing the study. The
confidentiality of their personal identities was
assured.
The interview guide, developed through a
comprehensive literature review and
translated into the local language Kannada by
a specialized translator, included questions
such as: “Can you describe what menstruation
is and how you learned about it?”, “What
sources of information or education about
menstruation are available to you in your
community?”, “Do you have access to clean
and private facilities for changing and
disposal?”, and “Have you encountered any
myths or taboos related to menstruation, and
how do they affect your daily life?” Additional
prompts were used to elicit further
clarification. The interviews were audio
recorded and transcribed, with an average
duration of two hours.
Data analysis included interviews with all 32
participants. For participants who
communicated in Kannada, the researcher
translated the audio-recorded transcriptions
i nto English. The following steps were
employed to analyse the data using thematic analysis:
1. Thoroughly read the transcripts to ensure
a comprehensive understanding of the
details.
2. Developed codes based on identified
commonalities.
3. Identified all potential themes and sub
themes.
4. Reviewed the identified themes to ensure
they accurately represent the dataset.
5. Label the themes with clear and precise
descriptions.
6. Articulated the narratives derived from the
data analysis in a clear and compelling
manner in the final report (Clarke & Braun,
2017).
Before analysis, all information collection
involved field notes, observations, reflections,
interviews, and audio or visual recordings.
Interviews were transcribed to create textual
data for analysis. NVivo software was used
for data management, coding, and theme
generation.
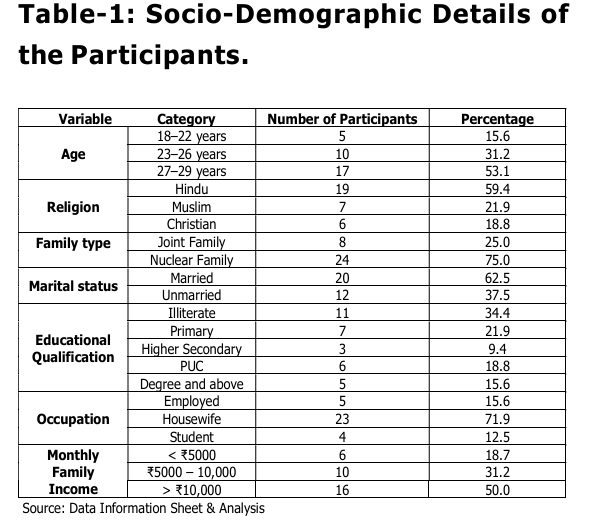
Table-1: provides the socio-demographic
characteristics of the 32 participants. The
majority of participants (53.13%) were late
youth, aged 27-29, while 31.25% were
emerging youth, aged 23-26, and the
remaining 15.63% were early-aged youth (18
22 years). Most participants identified as
Hindu (59.4%), followed by Muslim (21.9%)
and Christian (18.8%). The majority lived in
nuclear families (75%) and were married
(62.5%). Notably, a significant number
(34.4%) were illiterate, indicating potential
barriers to accessing information on menstrual
health. Occupation-wise, most participants
were housewives (71.9%), and the majority
had a monthly family income greater than ¹
10,000 (50.0%)
The analysis followed Braun and Clarke’s
(2006) six-phase framework for thematic
analysis, ensuring a rigorous approach to
identifying, coding, and validating key themes
from the data (Nowell et al., 2017; Clarke &
Braun, 2017). The interview transcripts were
read and re-read to familiarize researchers
with the content, noting recurring concepts.
A line-by-line coding approach was used to
group meaningful text segments into
descriptive and interpretative codes. These
codes were then organized into broader
themes, such as “Access to Menstrual Hygiene
Products” and “Menstrual Knowledge.” Themes
were refined for coherence, and sub-themes
were identified for additional detail. Two
independent researchers coded the data,
achieving high inter-coder reliability (Cohen’s
Kappa = 0.80) (McHugh, 2012). Participant
validation (a subset of participants, n = 5)
further enhanced credibility through member
checking. The qualitative data were analyzed
under six key identified themes: Menstrual
Knowledge and Awareness, Access to
Menstrual Hygiene Products, Hygiene
Practices, Privacy and Facilities, Stigma and
Myths, and Health and Well-being.
Participants exhibited and shared a range of
understanding about menstruation, from
accurate knowledge to misconceptions. Most
relied on family members, particularly
mothers, for information, but knowledge was
often incomplete.
Information sources included formal
education, community discussions, and family
teachings. However, inconsistencies in the
depth and accuracy of information across
sources affected the participants’
understanding.
“I was not aware of this before going to the
hostel; it was my mother who informed me.
It was an unexpected and quiet transition into
womanhood. Growing up in the Siddi tribal
community, discussions about menstruation
were rare. It was not something we talked
about openly, and information was limited. My
mother’s guidance became crucial but
meanwhile insufficient.”
Participants reported varied experiences
regarding access to menstrual products, with
some using commercial sanitary pads while
others relied on homemade alternatives due
to limited availability in their communities.
Barriers to accessing menstrual hygiene
products included limited availability in local
shops and a lack of awareness about
affordable options, particularly within the
Siddi Tribal community.
“It is very difficult to access menstrual hygiene
products. Availability in our Siddi community
is discouragingly limited. The scarcity in local
shops compounds the challenge, making it
especially difficult for us in this area.”
Participants’ menstrual hygiene practices
varied significantly, with some maintaining
regular cleaning routines, while others
struggled to follow consistent hygiene
practices.
Participants reported different routines
regarding changing sanitary products. While
some changed pads frequently, others relied
on reusable clothes, which were changed
infrequently.
“In my daily routine, I change sanitary pads
or products about 3-4 times a day to maintain
cleanliness and comfort. I make it a point to
clean myself thoroughly twice a day, ensuring
hygiene is a priority. Taking a bath and
following a regular routine contribute to my
overall well-being during menstruation.”
“In my daily routine, I rarely use pads or
products, often relying on clothes that I
replace only once or twice. I usually clean
myself thoroughly in the morning, but hygiene
is not a priority at other times of the day.
Occasionally, I skip baths when I am busy with
household chores.”
Privacy and access to appropriate facilities for managing menstrual hygiene were major
concerns, especially for those living in shared
spaces.
Some participants reported difficulties in
finding private spaces for changing menstrual
products, especially in public or communal
settings, affecting their comfort during
menstruation.
“Maintaining privacy during menstruation is a
significant challenge in our Siddi community.
In shared living spaces, finding a moment of
solitude is difficult. The struggle becomes
more pronounced when it comes to changing
re-usable clothes, pads or managing personal
hygiene.”
Participants shared experiences of cultural
stigma and myths surrounding menstruation,
which often dictated behaviour and reinforced
taboos.
Cultural beliefs influenced the way
menstruation was perceived and managed,
with practices such as isolation during
menarche being common. These practices
affected participants’ sense of normalcy
during their menstrual cycles.
“In our culture, certain concerning practices
emerge when a girl reaches menarche. On
the first day, we are confined to a separate
room, barred from entering the home or
participating in various activities and festivals A new bathroom is also constructed
exclusively for us, meant for our use only.
However, after the fifth day of the menstrual
cycle, this bathroom is closed off, making it
impractical. These deeply rooted practices
have a significant impact on our daily lives.”
Participants reported both physical and
emotional health concerns related to
menstruation, highlighting the link between
menstrual hygiene and overall well-being.
Lack of access to resources and proper
hygiene often led to discomfort, infections,
and emotional distress. Participants
emphasized the need for improved menstrual
education and access to hygiene products to
mitigate these health risks.
“Health issues during menstruation are a
major concern in our Siddi community. The
lack of proper awareness and limited access
to resources exacerbate these challenges.
Women and girls often face discomfort,
infections, and emotional distress.”
Addressing menstrual hygiene behaviours
necessitates a nuanced understanding of
menstrual knowledge and awareness. Our
study uncovered a significant deficiency in
menstrual knowledge within the Siddi Tribal
Community. Our data indicated that while the
majority of women reported normal menstrual
cycles, some experienced irregularities,
specifically longer-than-usual gaps, which
may suggest underlying medical concerns.
None of the participants had a comprehensive
understanding of menstruation prior to its onset, with many perceiving it as the body’s
method of expelling “dirty blood” to prevent
infections. A substantial proportion of the
women were unaware of menstruation before
their first period, with friends being the
primary source of information. Other sources
included mothers and close relatives, while
online programs or advertisements were not
cited, likely due to the limited availability of
electricity in Siddi villages. Dhingra et al.
(2009) found similar results and reported that
menstruation, known locally as “Kapadaanna”
or “Mahavari,” was not fully understood by
young adolescents before its onset. The girls
viewed it as essential for removing “dirty
blood” to prevent infections or diseases.
These challenges reinforce the observations
and calls for enhanced efforts to address the
barriers to menstrual hygiene product
availability.
Our findings show culture and social stigma
are associated with menstruation. These
findings align with Garg and Anand (2015),
showing that cultural beliefs associating
menstruation with impurity lead to various
restrictions for girls and women. Women are
often barred from the “puja” room and face
kitchen restrictions. Menstruating women are
also prevented from offering prayers or
touching holy books due to beliefs about
contamination. Kumar and Srivastava (2011)
noted the unfounded belief that menstruation
emits a smell or ray that spoils preserved
food. Traditional taboos linking menstruation
to evil spirits and practices like burying
menstrual cloths persist in some cultures,
including parts of Asia, despite lacking
scientific basis.
Maintaining privacy during menstruation is a
significant challenge in the Siddi community.
These results align with Mudi et al. (2023),
who found that privacy concerns during
menstruation in tribal communities are deeply
tied to cultural practices. Menstrual cloths are
often concealed under other laundry,
reflecting shame and stigma. The reuse of the
same cloth and poor drying methods increase
infection risks. Traditional beliefs, such as
avoiding baths or handling food during
menstruation, further complicate menstrual
hygiene, exacerbated by limited knowledge
and the perception of menstruation as a divine
curse. Such restrictions and stigma contribute
to increased anxiety, depression, reduced
self-esteem and overall psychological
wellbeing among women.
Our study found minimal use of disposable
absorbents or pads among disadvantaged
groups in the Siddi Tribe, consistent with Ram
et al. (2020). This disparity underscores
systemic challenges that limit access to
essential menstrual hygiene products. Low
usage among marginalized communities is
driven by restricted access, financial
constraints, and cultural norms, compounded
by a lack of menstrual health education. The
preference for reusable old clothes over
sanitary pads among tribal women is driven
by cost, availability, and disposal concerns.
According to Kumari et al. (2021), while child
marriage has a long history in India, it is not
prevalent across all social groups, particularly
among tribal populations. In these tribes,
marrying biologically immature girls is
uncommon, as marriage is intended to fulfill
the couple’s sexual needs. Puberty serves as
a significant milestone, with marriage typically
occurring within 2–6 years after menarche.
Consequently, early menarche may result in
early marriage (Kumari et al., 2021).
However, within the Siddi tribe, marriages
often take place at peak youth age, between
20 to 25 years, with a minimal gap between
menarche and marriage.
Literature indicates low usage of disposable
absorbents,
especially
among
socioeconomically disadvantaged groups,
highlighting an urgent need for targeted
interventions. Strategies should focus on
raising awareness and improving access to affordable disposable pads. Educating women
about the health risks of non-disposable
products is vital, and integrating menstrual
hygiene discussions into routine health worker
visits is necessary to increase usage. The
impact of media in promoting disposable
absorbents is evident, as those with limited
media exposure use them less. Strengthening
outreach and developing targeted programs
for disadvantaged groups, along with
supporting campaigns like “18 to 82” (which
seeks to bridge the gap between the 18% who
use sanitary napkins and the 82% who engage
in unhygienic practices) and Run4Nine (which
strives to ensure no woman or girl is
disadvantaged due to her biology), are
essential. Expanding initiatives such as
Menstrual Hygiene Day induce promoting
menstrual hygiene awareness with support
from celebrities. Social marketing approaches
similar to those in reproductive health could
boost disposable absorbent use. Platforms like
Rashtriya Kishor Swasthya Karyakram should
integrate menstrual hygiene with adolescent
health initiatives (MoHFW, 2014). Increasing
the availability of affordable products is also
crucial, as shown by Uttar Pradesh’s low
availability and high prices. Directing health
workers to distribute subsidised pads and
expanding school-based programs could
significantly improve access.
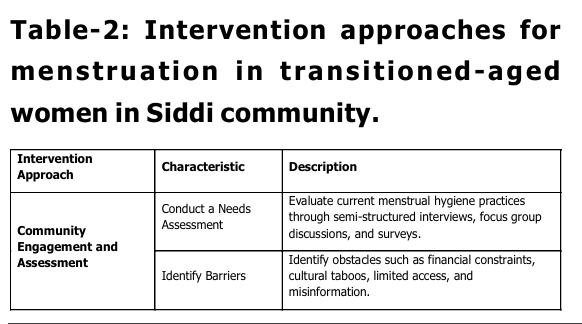
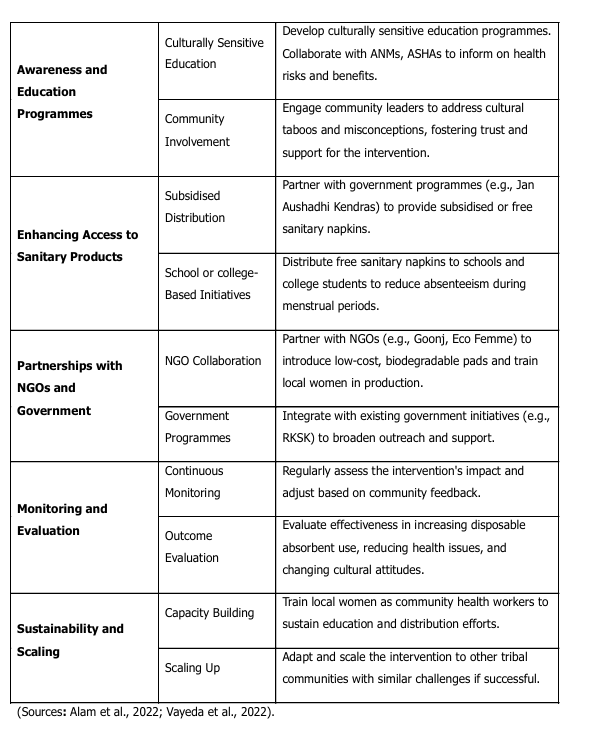
Empowering the Siddi tribe with a
collaborative approach to transform menstrual
hygiene through education, access, and
sustainable intervention (Table-2).
The study underscores the significant need
for targeted strategies to enhance menstrual
hygiene among transition-aged women in the
Siddi Tribal Community. These strategies
should encompass educational outreach,
subsidized sanitary products, and
strengthened support from frontline health
workers. The research reveals significant
gaps in menstrual knowledge, often worsened
by insufficient education and family support,
which contribute to widespread
misconceptions and poor hygiene practices,
leading to both physical and emotional health
issues. Limited access to menstrual products,
particularly in local markets, further
complicates the situation, highlighting the
critical need for reliable and affordable
options. Additionally, cultural norms and
taboos hinder open discussions about
menstruation, while challenges in maintaining
privacy in shared living environments
underscore the necessity for culturally
sensitive solutions. Traditional practices surrounding menarche play a significant role
in daily life, necessitating integrated strategies
supported by well-designed policies and
programs. These interventions should include
comprehensive, culturally relevant educational
initiatives that not only empower women but
also honour traditional values. The study also
highlights the psychological impact of reusing
menstrual products to conceal bloodstains,
linking the low use of disposable absorbents
to socio-economic challenges and a sense of
disempowerment. Addressing these issues
through targeted interventions is crucial for
improving menstrual hygiene, reducing school
or college absenteeism, and fostering both
economic and social empowerment within the
community.
Acknowledgment
We are deeply appreciative of the participants
for sharing their knowledge and experiences
about menstruation. We extend our sincere
thanks to the Siddi community for their
invaluable support and insights into Siddi
cultural practices and environmental factors.
Alam, M. U., Sultana, F., Hunter, E. C., Winch,
P. J., Unicomb, L., Sarker, S., … &
Luby, S. P. (2022). Evaluation of a
menstrual hygiene intervention in
urban and rural schools in Bangladesh:
a
pilot
study. BMC Public
Health, 22(1), 1100.
Clarke, V., & Braun, V. (2017). Thematic
analysis. The journal of positive
psychology, 12(3), 297-298.
Dar, D. R., & Sobhana, H. (2024). Echoes of
Transition: Youth Mental Health in
Crossroads. IAPS Journal of Practice
in Mental Health, 2(1), 20-22.
Dhingra, R., Kumar, A., & Kour, M. (2009).
Knowledge and practices related to
menstruation among tribal (Gujjar)
adolescent girls. Studies on Ethno
Medicine, 3(1), 43-48.
Garg, S., & Anand, T. (2015). Menstruation
related myths in India: strategies for
combating it. Journal of family
medicine and primary care, 4(2), 184
186.
Kumar, A., & Srivastava, K. (2011). Cultural
and social practices regarding
menstruation among adolescent
girls. Social work in public
health, 26(6), 594-604.
Kumari, S., Sood, S., Davis, S., & Chaudhury,
S. (2021). Knowledge and practices
related to menstruation among tribal
adolescent girls. Industrial Psychiatry
Journal, 30(Suppl 1), S160-S165.
McHugh, M. L. (2012). Interrater reliability:
t he kappa statistic. Biochemia
medica, 22(3), 276-282.
Mishra, P. (2020). Periods, perceptions and
practice-a study of menstrual
awareness among adolescent girls in
a tribal district of Odisha, India. Indian
Journal of Public Health Research &
Development, 11(6), 577-585.
MoHFW. (2014). strategy handbook. https://
nhm.gov.in/images/pdf/programmes/
rksk-strategy-handbook.pdf
Mudi, P. K., Pradhan, M. R., & Meher, T. (2023).
Menstrual health and hygiene among
Juang women: a particularly
vulnerable tribal group in Odisha,
India. Reproductive Health, 20(1), 55.
Nowell, L. S., Norris, J. M., White, D. E., &
Moules, N. J. (2017). Thematic
analysis: Striving to meet the
trustworthiness criteria. International
journal of qualitative methods, 16(1),
1609406917733847.
Ram, U., Pradhan, M. R., Patel, S., & Ram, F.
(2020). Factors associated with
disposable menstrual absorbent use
among young women in
India. International Perspectives on
Sexual and Reproductive Health, 46, 223-234.
Sivakami, M., van Eijk, A. M., Thakur, H.,
Kakade, N., Patil, C., Shinde, S., … &
Phillips-Howard, P. A. (2019). Effect
of menstruation on girls and their
schooling, and facilitators of
menstrual hygiene management in
schools: surveys in government
schools in three states in India,
2015. Journal of global health, 9(1).
Torondel, B., Sinha, S., Mohanty, J. R., Swain,
T., Sahoo, P., Panda, B., … & Das, P.
(2018). Association between
unhygienic menstrual management
practices and prevalence of lower
reproductive tract infections: a
hospital-based cross-sectional study
i n Odisha, India. BMC infectious
diseases, 18, 1-12.
Upashe, S. P., Tekelab, T., & Mekonnen, J.
(2015). Assessment of knowledge and
practice of menstrual hygiene among
high school girls in Western
Ethiopia. BMC women’s health, 15, 1
8.
Vayeda, M., Ghanghar, V., Desai, S., Shah, P.,
Modi, D., Dave, K., … & Shah, S.
(2022). Improving menstrual hygiene
management among adolescent girls
i n tribal areas of Gujarat: an
evaluation of an implementation model
integrating the government service
delivery system. Sexual and
Reproductive Health Matters, 29(2),
1992199.
WHO. (2023, October 3). Sanitation. WHO;
World Health Organization: WHO.
https://www.who.int/news-room/
fact-sheets/detail/sanitation