
Indian Journal of Health Social Work
(UGC CARE List Journal)
LIFESTYLE DISEASES AND QUALITY OF LIFE
Kalpana Singh
Senior Research Fellow, Department of Sociology, Dayanand Brajendra Swarup P.G.
College, Kanpur
Correspondence: Kalpana Singh, e-mail: kalpana.sengar10@gmail.com
ABSTRACT
Lifestyle diseases, especially non-communicable diseases (NCDs) are rising at an alarming rate
and are clearly visible in developed as well as developing countries too. The shift in the mode of
production from agriculture to industrial and towards rising service sectors has brought significant
changes in lifestyle and considerably altered daily routines, eating habits, food choices and overall
health. NCDs including cardiovascular diseases, obesity, type 2 diabetes, malnutrition and more
are interlinked to unhealthy lifestyles and their effect, treatment and post-maintenance varies
across different socioeconomic classes. The branch of sociology, medical sociology dives into
the intersection of health, illness and socioeconomic factors, and every health policy needs this
dimension into consideration for output. This research paper is based on analyses of primary
data collected from individuals suffering from NCDs and secondary data published online (NFHS
5, Government, WHO). The findings emphasize the early intervention of government, organizations,
and civil society at an early stage and the need to work more towards preventing NCDs rather
than cure at later stages of diseases, by incorporating traditional and non-conventional medicine
practices and mass awareness programs.
Keywords: Lifestyle diseases, Non-communicable Diseases, Risk factors, Socioeconomic factors,
Public health policy.
Submitted: 14.07.2025 Revised: 28.08.2025 Accepted: 19.09.2025 Published: 28.01.2026
How to cite this article: Singh, K. (2025). Lifestyle diseases and quality of life. Indian Journal
of Health Social Work, 7(2), 75-84
INTRODUCTION
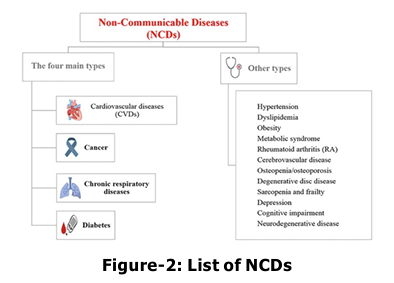
Non-communicable diseases are termed life l ong diseases collectively affected by environmental, physiological and behavioural factors. NCD treatment needs prolonged medication and today individuals from both high socio-economic backgrounds and marginal sections are affected by it. It includes a variety of diseases, including cardiovascular diseases (such as heart disease and stroke), diabetes, certain inherited genetic disorders, various types of cancer, reproductive health issues, poor nutrition, obesity, and more. Social determinants of health (SDOH) play a crucial role in shaping individual and population health outcomes. These determinants are the conditions in which people are born, grow, live, work, and age, and they are influenced by the distribution of resources, power, and money at various levels—global, national, and local. Diseases which were heard after the 60s and 70s among individuals are visible today in early 20s and 30s of a person. To what extent change in lifestyle can impact in early prevention of NCDs is a rising concern of governments. The chief reason behind this is even if the government increase hospitals, medical practitioners, and other associated infrastructure, it is not possible to cure every individual suffering from NCDs and people are generally visit hospitals in the later stages of diseases which increases the cost of cure, risk and decreases chances of survival. Another significant issue is if the majority of the workforce in any country which is assumed to be aged between 15-59 (India) years, gets trapped in a lifelong cycle of diseases, medication, and survival then how will they contribute to the economy and development? Research indicates that risk factors for non communicable diseases are notably concentrated among individuals aged 30-49, particularly those with poor social determinants such as low educational attainment, marital separation, and adverse socioeconomic backgrounds, compounded by poorly structured work environments in urban settings. This demographic is poised to exert increased pressure on public health centres, necessitating intervention strategies from policymakers. Furthermore, data reveal that individuals from lower socioeconomic strata exhibit a higher propensity for tobacco use, alcohol consumption, and suboptimal dietary practices, characterized by a lack of fruits and vegetables. Conversely, those from higher socioeconomic groups tend to demonstrate greater physical inactivity and a higher intake of unhealthy fats, sodium, and processed foods. Interestingly, a contrasting pattern emerges regarding the prevalence of heart disease and its associated risk factors, which are more pronounced in higher socioeconomic cohorts, coinciding with elevated mortality rates. Public health policy must prioritize equitable distribution and accessibility of healthcare resources to address the needs of the majority effectively. Additionally, the incidence of metabolic syndrome is found to be disproportionately higher among females, with contributing factors including advanced age, female gender, obesity, inadequate fruit intake, elevated cholesterol levels, and, surprisingly, middle-to-high socioeconomic status. This underscores metabolic syndrome as a salient public health concern, even in economically disadvantaged regions of India, warranting targeted interventions and strategic solutions. Significantly, studies focusing on adolescents in school settings have uncovered concerning dietary practices, encompassing excessive fast-food consumption and experimentation with alcohol and tobacco, alongside rising rates of obesity and hypertension. Moreover, diabetes and hypertension have emerged as critical risk factors for chronic kidney disease, illustrating the interconnectedness of lifestyle diseases. Collectively, these findings highlight that once an individual becomes ensnared in the cycle of lifestyle-related diseases, the pathway to more complex health conditions is paved, severely affecting multiple organ systems. Implementing lifestyle modifications can play a crucial role in the prevention of these diseases.
Non-communicable diseases are termed life l ong diseases collectively affected by environmental, physiological and behavioural factors. NCD treatment needs prolonged medication and today individuals from both high socio-economic backgrounds and marginal sections are affected by it. It includes a variety of diseases, including cardiovascular diseases (such as heart disease and stroke), diabetes, certain inherited genetic disorders, various types of cancer, reproductive health issues, poor nutrition, obesity, and more. Social determinants of health (SDOH) play a crucial role in shaping individual and population health outcomes. These determinants are the conditions in which people are born, grow, live, work, and age, and they are influenced by the distribution of resources, power, and money at various levels—global, national, and local. Diseases which were heard after the 60s and 70s among individuals are visible today in early 20s and 30s of a person. To what extent change in lifestyle can impact in early prevention of NCDs is a rising concern of governments. The chief reason behind this is even if the government increase hospitals, medical practitioners, and other associated infrastructure, it is not possible to cure every individual suffering from NCDs and people are generally visit hospitals in the later stages of diseases which increases the cost of cure, risk and decreases chances of survival. Another significant issue is if the majority of the workforce in any country which is assumed to be aged between 15-59 (India) years, gets trapped in a lifelong cycle of diseases, medication, and survival then how will they contribute to the economy and development? Research indicates that risk factors for non communicable diseases are notably concentrated among individuals aged 30-49, particularly those with poor social determinants such as low educational attainment, marital separation, and adverse socioeconomic backgrounds, compounded by poorly structured work environments in urban settings. This demographic is poised to exert increased pressure on public health centres, necessitating intervention strategies from policymakers. Furthermore, data reveal that individuals from lower socioeconomic strata exhibit a higher propensity for tobacco use, alcohol consumption, and suboptimal dietary practices, characterized by a lack of fruits and vegetables. Conversely, those from higher socioeconomic groups tend to demonstrate greater physical inactivity and a higher intake of unhealthy fats, sodium, and processed foods. Interestingly, a contrasting pattern emerges regarding the prevalence of heart disease and its associated risk factors, which are more pronounced in higher socioeconomic cohorts, coinciding with elevated mortality rates. Public health policy must prioritize equitable distribution and accessibility of healthcare resources to address the needs of the majority effectively. Additionally, the incidence of metabolic syndrome is found to be disproportionately higher among females, with contributing factors including advanced age, female gender, obesity, inadequate fruit intake, elevated cholesterol levels, and, surprisingly, middle-to-high socioeconomic status. This underscores metabolic syndrome as a salient public health concern, even in economically disadvantaged regions of India, warranting targeted interventions and strategic solutions. Significantly, studies focusing on adolescents in school settings have uncovered concerning dietary practices, encompassing excessive fast-food consumption and experimentation with alcohol and tobacco, alongside rising rates of obesity and hypertension. Moreover, diabetes and hypertension have emerged as critical risk factors for chronic kidney disease, illustrating the interconnectedness of lifestyle diseases. Collectively, these findings highlight that once an individual becomes ensnared in the cycle of lifestyle-related diseases, the pathway to more complex health conditions is paved, severely affecting multiple organ systems. Implementing lifestyle modifications can play a crucial role in the prevention of these diseases.
METHODOLOGY
This research paper primarily used a qualitative content analysis methodological approach. Primary data have been collected from 15 respondents using purposive sampling. Their personal experiences were recorded via open-ended interviews and gathered narrative data from respondents. Among 15 female respondents who were facing multiple NCDs were selected. Among them 3 were aged between 11-30, 9 were aged between 31-49 and 3 were aged 60 and above. Interviews were conducted face-to face and lasted for an average of 45-50 minutes. Narratives were summarized keeping the respondent’s experience. Secondary data have been used extensively using government reports, NFHS-5 (National Family Health Surveys), and World Health Organization (WHO) publications, previous research studies and findings have been systematically analyzed to provide a comprehensive understanding of lifestyle diseases and their effect on quality of life. Ethical guidelines have been strictly followed.
This research paper primarily used a qualitative content analysis methodological approach. Primary data have been collected from 15 respondents using purposive sampling. Their personal experiences were recorded via open-ended interviews and gathered narrative data from respondents. Among 15 female respondents who were facing multiple NCDs were selected. Among them 3 were aged between 11-30, 9 were aged between 31-49 and 3 were aged 60 and above. Interviews were conducted face-to face and lasted for an average of 45-50 minutes. Narratives were summarized keeping the respondent’s experience. Secondary data have been used extensively using government reports, NFHS-5 (National Family Health Surveys), and World Health Organization (WHO) publications, previous research studies and findings have been systematically analyzed to provide a comprehensive understanding of lifestyle diseases and their effect on quality of life. Ethical guidelines have been strictly followed.
FINDINGS AND DISCUSSION
Existing health infrastructure in India Health facilities are increasing every year and India has covered several milestones. Yet there remain significant challenges and our governments have addressed them every time. There are several schemes related to individuals’ health across all ages and classes. One of them is the AYUSHMAN Bharat Yojana which is proving to be another milestone in this direction as the number of Ayushman cards made was 34.7 crore. In 2025 more investment seems to be directed towards novelty, AI and Robotics in the health sector. Today we have 780 medical colleges (431 government and 349 private), and seats in medical have risen to 1,18,137 for MBBS and 73,157 seats for Post Graduation. Out of GDP 1.9 per cent have been spent in 2023-24. Talking of the number of hospitals we have 2,00,988 health centers. The Maternal mortality rate has decreased to 103 per one lack is a significant achievement.
Existing health infrastructure in India Health facilities are increasing every year and India has covered several milestones. Yet there remain significant challenges and our governments have addressed them every time. There are several schemes related to individuals’ health across all ages and classes. One of them is the AYUSHMAN Bharat Yojana which is proving to be another milestone in this direction as the number of Ayushman cards made was 34.7 crore. In 2025 more investment seems to be directed towards novelty, AI and Robotics in the health sector. Today we have 780 medical colleges (431 government and 349 private), and seats in medical have risen to 1,18,137 for MBBS and 73,157 seats for Post Graduation. Out of GDP 1.9 per cent have been spent in 2023-24. Talking of the number of hospitals we have 2,00,988 health centers. The Maternal mortality rate has decreased to 103 per one lack is a significant achievement.
NCDS RISK FACTORS
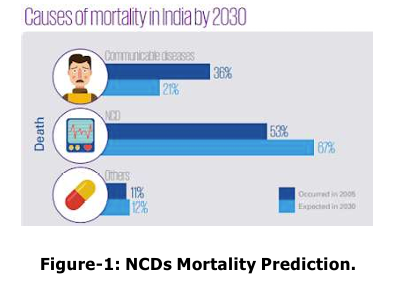
The proportion of mortality in India attributable to non-communicable diseases (NCDs) has escalated markedly, rising from 37.09 per cent in 1990 to 61.8 per cent in 2016. The incidence of cancer within India has shown a consistent annual increase, with cases expanding from 1,328,229 in 2014 to 1,517,426 in 2017. Correspondingly, cancer related mortality has also seen an upward trajectory, from 670,541 deaths in 2014 to 766,348 in 2017. Data from the 2015-16 National Family Health Survey (NFHS) indicates that hypertension affects 11 per cent of women and 15 per cent of men aged 15 to 49 years. In response to the rising burden of NCDs, the Indian government has implemented a series of strategic measures, notably the National Health Policy 2017. This policy prioritizes preventive and promotional healthcare initiatives and strives for universal access to quality healthcare services. It aims specifically at mitigating premature mortality from major NCDs, including cardiovascular diseases, cancer, diabetes, and chronic respiratory conditions. The National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) is operational under the National Health Mission, focusing on raising awareness about cancer prevention, early detection, and treatment modalities. NPCDCS places a particular emphasis on the prevention of breast, cervical, and oral cancers. As part of a comprehensive approach to primary healthcare under the National Health Mission, initiatives have been introduced across over 150 districts for the prevention, management, and screening of prevalent NCDs, including diabetes and hypertension, as well as oral, breast, and cervical cancers. Furthermore, six new All India Institutes of Medical Sciences (AIIMS) have been established via the Pradhan Mantri Swasthya Suraksha Yojana (PMSSY), enhancing tertiary care facilities for NCDs like diabetes. Additionally, a pilot initiative is currently being trialled in six districts in collaboration with the Ministry of AYUSH (Ayurveda, Yoga, Unani, Siddha and Homeopathy) to explore the potential contributions of AYUSH systems of medicine in the prevention and management of NCDs.
The proportion of mortality in India attributable to non-communicable diseases (NCDs) has escalated markedly, rising from 37.09 per cent in 1990 to 61.8 per cent in 2016. The incidence of cancer within India has shown a consistent annual increase, with cases expanding from 1,328,229 in 2014 to 1,517,426 in 2017. Correspondingly, cancer related mortality has also seen an upward trajectory, from 670,541 deaths in 2014 to 766,348 in 2017. Data from the 2015-16 National Family Health Survey (NFHS) indicates that hypertension affects 11 per cent of women and 15 per cent of men aged 15 to 49 years. In response to the rising burden of NCDs, the Indian government has implemented a series of strategic measures, notably the National Health Policy 2017. This policy prioritizes preventive and promotional healthcare initiatives and strives for universal access to quality healthcare services. It aims specifically at mitigating premature mortality from major NCDs, including cardiovascular diseases, cancer, diabetes, and chronic respiratory conditions. The National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) is operational under the National Health Mission, focusing on raising awareness about cancer prevention, early detection, and treatment modalities. NPCDCS places a particular emphasis on the prevention of breast, cervical, and oral cancers. As part of a comprehensive approach to primary healthcare under the National Health Mission, initiatives have been introduced across over 150 districts for the prevention, management, and screening of prevalent NCDs, including diabetes and hypertension, as well as oral, breast, and cervical cancers. Furthermore, six new All India Institutes of Medical Sciences (AIIMS) have been established via the Pradhan Mantri Swasthya Suraksha Yojana (PMSSY), enhancing tertiary care facilities for NCDs like diabetes. Additionally, a pilot initiative is currently being trialled in six districts in collaboration with the Ministry of AYUSH (Ayurveda, Yoga, Unani, Siddha and Homeopathy) to explore the potential contributions of AYUSH systems of medicine in the prevention and management of NCDs.
In India, in 2017 nearly 60 per cent of all
fatalities were directly related to NCDs. Risk
factors like tobacco consumption, alcohol,
unhealthy dietary habits, obesity, physical
i nactivity, high blood pressure, high
cholesterol level, heightened glucose level,
and high salt intake of an average of 11mg/
day against the WHO recommended 5mg/day.
Obesity is a growing health crisis in India.
Both obesity and undernutrition are forms of
malnutrition and are found in contrasting
socioeconomic groups. Globally the number
of obese has crossed 100 crores. In India,
statistics show number of overweight children
aged between 5 to 19 years exceeds 1.25
crore in 2022 compared to 40 lakhs in 1990,
which is a four times increase in obesity. One
person once diagnosed with one type of NCD
opens doors for other NCDs too.
Life is running at a fast pace and to fill
stomachs fast options calming the taste buds
is also growing in demand. The fast-food
market has grown to 731 billion dollars in
2022. The United States leads the
consumption ladder with annual spending of
160 billion dollars, followed by China with 97
per cent of the population consuming fast
food. India ranks 13th on this ladder with an
annual fast-food revenue of 814.29 million
USD in 2023. According to The Global Food
Policy Report 2024: Food Systems for Healthy
Diets and Nutrition, published by the
International Food Policy Research Institute
(IFPRI) on May 29 a healthy diet consists of
incorporating 5 food groups in the diet that
is, staple food, vegetable, fruit, pulses, nut
or seed, animal source food). Only 28 per cent
of Indians are following this defined healthy
diet. Modern lifestyle has incorporated
sedentary ways of doing daily activities, even
the recreational activities are limited to
reduced physical activity. Behaviours include
a prolonged session of watching television,
mobile screens, laptops, using electronic
devices, and video gaming. The work culture
associated with service sectors requires
elongated hours of sitting at one go of an
average of 10-11 hours per day. School
curriculum and increasing competitions and
cutthroat race to secure a seat and position
also demand long hours of sitting. Modular
kitchens with all appliances and raised cooking
platforms as opposed to traditional kitchens
with sitting and cooking arrangements make
people stand in one place during entire
cooking and associated works with little
mobility. Global study reveals high levels of
physical inactivity among women as compared
to men. This is associated with small families, small residences with modern means of
machinery and luxuries within the home,
availability of maids and more eating done
either outside the home or via online food
delivery companies. The online food delivery
market in India in 2023 was 36.3 billion dollars
with a growth rate of 24.32 per cent. Above
these increasing subscriptions to digital
platforms like Netflix, Amazon Prime and
similar others have grown to 73 billion Indian
rupees, showing time consumed in screen
based activities. Next on the list is the
increasing trend towards online shopping and
associated screen time scrolling up and down
for not only essentials or needed items at that
particular time, but also looking for the best
deals, discounts and offers which in turn
consumes a lot of time and contributes
towards more sitting hours, as individuals are
spending and an average of 2 hours and 25
minutes per week and spending 16 per cent
of their income to this activity (consumer study
by CyberMedia Research, CMR). This trend is
not just limited to metropolitan cities but has
percolated to tier 2 and tier 3 cities and rural
areas as well. This situation is exacerbated
by the post-pandemic circumstances
characterized by prolonged sitting and remote
operated work arrangements.
The use of alcohol and tobacco is an emerging
leading risk factor for mortality in India.
Tobacco only resulted in 1 million deaths (17.8
per cent of total deaths). Smoking accounted
for 79.8 per cent of these fatalities, with
secondhand smoke contributing 21.0 per cent.
Major causes of mortality linked to tobacco
include Ischemic Heart Disease (18.0 per
cent), Stroke (14.2 per cent), Lung Cancer
(60.4 per cent), and Chronic Obstructive
Pulmonary Disease (40.7 per cent). The
increased prevalence of cigarette smoking and
alcohol consumption among adolescents is
influenced by parental habits, peer pressure,
experimentation, imitating the cool images of
actors on big screens, lack of family cohesion,
inadequate parental supervision, and no
quality family time due to busy lifestyles.
Collectively these conditions foster a sense
of loneliness, and fear of failure which further
compound the issue. Food and beverage
companies invest significantly huge amounts
in advertisements and popularizing brands
and very little attention is given to nutritional
content and healthy choices for the public at
large. Social influencers also contribute
t owards building public opinions and
i ncreasing party habits, celebrating in
restaurants and food outlets and changing the
way people live their lives. FMCG (Fast-moving
consumer goods) sector topped the list of
advertisement spending with 300 billion Indian
rupees in 2023 (Statista.com).
The last section is about the factors which
are beyond individual control. Top in the list
is the issue of poor air quality index (AQI),
that harms multiple organ systems. This
situation has worsened up in metropolitan
cities across the world and caused 5,00,000
lung cancer and 1.6 million COPD (Chronic
Obstructive Pulmonary Disease) deaths
annually, 19 per cent cardiovascular and 21
per cent of stroke deaths. Development
induced pollution has shrinked access to
affordable open and green spaces for all age
groups. Poor urban development plans and
mass migrated population from lower strata
of society are bound to live in slums, with no
fresh air, no ventilation, sunlight not able to
reach ground, unhygienic living conditions and
lack of sanitation put them at door of NCDs.
The demographic effects of air pollution reveal
distinct disparities: families from high socio
economic background often escape to natural
environments such as beaches and hill
stations, utilizing their resources to mitigate
exposure to pollutants. Conversely, individuals
from middle-income groups tend to invest in
air purification technologies for their homes
and vehicles, attempting to create cleaner
environments within confined spaces. In stark contrast, those from lower socio-economic
strata disproportionately bear the brunt of air
pollution’s adverse health impacts, with
prolonged exposure leading to severe
respiratory ailments. Essential infrastructure,
such as playgrounds for children, walking
paths for adults, and activity spaces for the
elderly, is insufficiently provided in
increasingly congested urban environments.
As urban populations continue to rise,
affordable and adequate housing remains a
critical challenge, often relegating
communities in affluent areas may offer the
necessary amenities, yet skyrocketing real
estate prices render these options
inaccessible to both middle-class and lower
i ncome
populations.
The
mere
acknowledgement of the right to life within
constitutional frameworks does not ensure a
viable standard of living for all citizens. There
is an urgent need for sustainable urban
planning and housing initiatives that provide
dignified living conditions for everyone,
supported by proactive government policies
and interventions.
Personal Experience of a Respondent
“I’m Sarla Devi (name changed), a 60-year
old woman who has been battling type 2
diabetes since my early 40s. Sleep eludes me,
and I often rely on sleeping pills to get by.
After an accident at 45, which left me with
multiple fractures in my leg, my mobility
declined, and I started gaining weight, leading
to serious health issues like obesity,
inflammation, and heart problems. I now
depend on insulin and my elder son for help
with daily tasks. Although my relatives live just
200 meters away, I struggle to visit them
without assistance. My family checks in on me
often, but I still face a lot of psychological
and physical challenges. Coming from a
respectable family, I never thought I would
feel so dependent on others. Visits from
relatives are infrequent, and even the ones
who come find it hard to help. While my
medical expenses aren’t a major issue due to
my socioeconomic status, I often feel trapped
in this cycle of illness, which has contributed
to a negative self-image and mood swings.
My day starts at 4 a.m., I sit lost in thought,
trying to prepare my morning tea. I find myself
relying on others for basic needs like drinking
water, and my son has to give me my insulin
injections. This routine has been my life for
over two decades, and watching other women
my age live freely only deepens my feelings
of isolation and longing for a different life.”.
“My name is Riya Chakraborty (name changed)
and I am 14 years old. I suffer from obesity
and was later diagnosed with asthma, which
means I have to carry a small inhaler pump
with me at all times. This has limited my
participation in sports and other activities,
leading to the development of a negative self
image.”
Socioeconomic Factors and their relation
to Non-Communicable Diseases (NCDs)
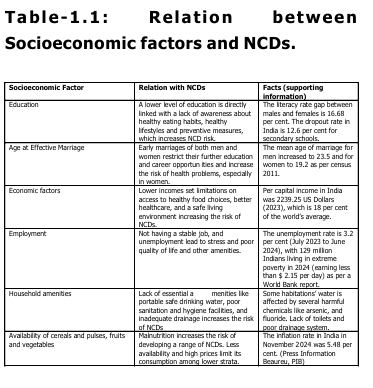
Socioeconomic factors are deeply connected to the spread and prevention of risks associated with NCDs as summarized in the following table 1.1 given below.
Socioeconomic factors are deeply connected to the spread and prevention of risks associated with NCDs as summarized in the following table 1.1 given below.
CONCLUSION
Gandhi’s stand on health
In 2022, approximately 7.5 million people were diagnosed with hypertension, 6.1 million with diabetes, and 2.9 million with both hypertension and diabetes. Additionally, 200,000 peopl e were diagnosed with cardiovascular diseases (CVDs), 100,000 with stroke, and 300,000 with common cancers. The average out-of-pocket spending by households on non-communicable diseases (NCDs) in public hospitals was INR 13,170. The economic burden posed b y NCDs is estimated to result in a global cumulative economic loss of $47 trillion between 2011 and 2030. This significant loss hinders economic development and perpetuates poverty. Gandhi’s key suggestions for a healthy lifestyle focus on several important aspects: he advocated for an appropriate diet that is balanced and limits high substances like fats, carbohydrates, and salt, while also endorsing fasting for detoxification. He emphasized the need for regular physical activity to mitigate the risks of a sedentary lifestyle, encouraged avoiding tobacco and alcohol due to their health consequences, and highlighted the i mportance of breathing clean air and 3maintaining a clean environment. These principles address significant risk factors for non-communicable diseases (NCDs) and reflect Gandhi’s revolutionary philosophy on health, which remains relevant in today’s fight against the NCD epidemic. Mahatma Gandhi conveyed that the body was never meant to be treated as a refuse bin, holding all the foods that the palate demands. He recognized that physical training should have as much place in the curriculum as mental training. Gandhi stated that havoc has been created for mankind by tobacco, and he noted that those who take to drinking ruin themselves and their people, as expressed in Key to Health (1948). He regarded air, water, and grains as the three chief kinds of food, and highlighted that when air is polluted, our health is harmed; it is said that bad air is more harmful than bad water. Gandhi emphasized that instead of being used as a temple of God, the body is often treated as a vehicle for indulgences, with individuals rushing to medical men for help. He believed that true wealth lies in health, rather than in pieces of gold and silver
Gandhi’s stand on health
In 2022, approximately 7.5 million people were diagnosed with hypertension, 6.1 million with diabetes, and 2.9 million with both hypertension and diabetes. Additionally, 200,000 peopl e were diagnosed with cardiovascular diseases (CVDs), 100,000 with stroke, and 300,000 with common cancers. The average out-of-pocket spending by households on non-communicable diseases (NCDs) in public hospitals was INR 13,170. The economic burden posed b y NCDs is estimated to result in a global cumulative economic loss of $47 trillion between 2011 and 2030. This significant loss hinders economic development and perpetuates poverty. Gandhi’s key suggestions for a healthy lifestyle focus on several important aspects: he advocated for an appropriate diet that is balanced and limits high substances like fats, carbohydrates, and salt, while also endorsing fasting for detoxification. He emphasized the need for regular physical activity to mitigate the risks of a sedentary lifestyle, encouraged avoiding tobacco and alcohol due to their health consequences, and highlighted the i mportance of breathing clean air and 3maintaining a clean environment. These principles address significant risk factors for non-communicable diseases (NCDs) and reflect Gandhi’s revolutionary philosophy on health, which remains relevant in today’s fight against the NCD epidemic. Mahatma Gandhi conveyed that the body was never meant to be treated as a refuse bin, holding all the foods that the palate demands. He recognized that physical training should have as much place in the curriculum as mental training. Gandhi stated that havoc has been created for mankind by tobacco, and he noted that those who take to drinking ruin themselves and their people, as expressed in Key to Health (1948). He regarded air, water, and grains as the three chief kinds of food, and highlighted that when air is polluted, our health is harmed; it is said that bad air is more harmful than bad water. Gandhi emphasized that instead of being used as a temple of God, the body is often treated as a vehicle for indulgences, with individuals rushing to medical men for help. He believed that true wealth lies in health, rather than in pieces of gold and silver
Early Intervention Strategies for
Preventing Non-communicable Diseases
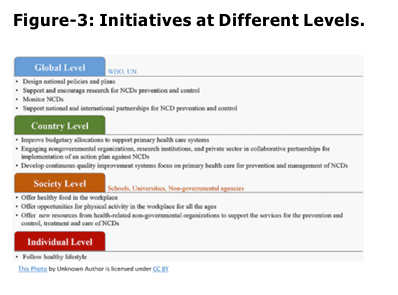
We need to incorporate healthy lifestyles, food habits, and health well-being, and this issue needs immediate attention from the government, organizations, civil society, media, and schools. Our traditional and non conventional medicinal practices, system and knowledge (AYUSH- Ayurveda, Yoga, Unani, Siddha, and Homeopathy) can play a significant role, through the adoption of balanced diets and active living. Ayurveda has deep historical connections to the principles of nutrition and is gaining recognition globally as a viable option for managing lifestyle related disorders. Among its key practices are Panchakarma and Rasayana, both of which emphasize the importance of detoxification and rejuvenation of the body. Dietary control, alongside physical practices like Ashtanga Yoga, plays a pivotal role in regulating the senses and enhancing mental focus. The government can also act in several ways taking cues from other countries on putting checks on salty snacks and fast food by imposing heavier taxes on them. FSSAI (Food Safety and Standards Authority of India) needs to expand its base, increase the frequency of quality checks on packed food items and famous food outlets and impose severe penalties for substandard deliveries to consumers. Workshops should be conducted in schools starting from the eighth grade, empowering young individuals to become health ambassadors in their communities. Online food deliveries also need to be put under surveillance as they promise 10 minutes but not the quality of food being delivered. Whether the population opt for closed or paid gyms estimated to be around 96,278, free and open gyms have made fitness affordable and accessible to the masses, children’s parks, sports clubs or walking paths, have options and facilities for all. Lastly, it would be valuable to develop simple meal plans that include regional variations and seasonal foods, which can be taught in educational institutions and widely circulated. By fostering an environment where healthy, simple lifestyles are the norm, we can take significant strides towards reducing the burden of lifestyle diseases in our communities. Healthcare Schemes in India, Non Communicable Diseases (https://pib.gov.in) The National Tobacco Control Programme (NTCP) aims to reduce tobacco use, while the NPCDCS addresses non-communicable diseases such as cancer and diabetes. Specific health initiatives include programs for occupational diseases, hearing impairment, and mental health, the latter through the National Mental Health Programme. Vision care is enhanced via the NPCB&VI, and renal needs are met through the Pradhan Mantri National Dialysis Programme (PMNDP). The National Programme for Health Care for the Elderly (NPHCE) focuses on older adults, and the National Programme for Prevention and Management of Burn Injuries (NPPMBI) addresses burn injuries. Additionally, the National Oral Health Programme promotes better dental health across the population.
We need to incorporate healthy lifestyles, food habits, and health well-being, and this issue needs immediate attention from the government, organizations, civil society, media, and schools. Our traditional and non conventional medicinal practices, system and knowledge (AYUSH- Ayurveda, Yoga, Unani, Siddha, and Homeopathy) can play a significant role, through the adoption of balanced diets and active living. Ayurveda has deep historical connections to the principles of nutrition and is gaining recognition globally as a viable option for managing lifestyle related disorders. Among its key practices are Panchakarma and Rasayana, both of which emphasize the importance of detoxification and rejuvenation of the body. Dietary control, alongside physical practices like Ashtanga Yoga, plays a pivotal role in regulating the senses and enhancing mental focus. The government can also act in several ways taking cues from other countries on putting checks on salty snacks and fast food by imposing heavier taxes on them. FSSAI (Food Safety and Standards Authority of India) needs to expand its base, increase the frequency of quality checks on packed food items and famous food outlets and impose severe penalties for substandard deliveries to consumers. Workshops should be conducted in schools starting from the eighth grade, empowering young individuals to become health ambassadors in their communities. Online food deliveries also need to be put under surveillance as they promise 10 minutes but not the quality of food being delivered. Whether the population opt for closed or paid gyms estimated to be around 96,278, free and open gyms have made fitness affordable and accessible to the masses, children’s parks, sports clubs or walking paths, have options and facilities for all. Lastly, it would be valuable to develop simple meal plans that include regional variations and seasonal foods, which can be taught in educational institutions and widely circulated. By fostering an environment where healthy, simple lifestyles are the norm, we can take significant strides towards reducing the burden of lifestyle diseases in our communities. Healthcare Schemes in India, Non Communicable Diseases (https://pib.gov.in) The National Tobacco Control Programme (NTCP) aims to reduce tobacco use, while the NPCDCS addresses non-communicable diseases such as cancer and diabetes. Specific health initiatives include programs for occupational diseases, hearing impairment, and mental health, the latter through the National Mental Health Programme. Vision care is enhanced via the NPCB&VI, and renal needs are met through the Pradhan Mantri National Dialysis Programme (PMNDP). The National Programme for Health Care for the Elderly (NPHCE) focuses on older adults, and the National Programme for Prevention and Management of Burn Injuries (NPPMBI) addresses burn injuries. Additionally, the National Oral Health Programme promotes better dental health across the population.
Road Ahead
Governments can make significant contributions to containing NCDs by increasing t axes on unhealthy packed food and simultaneously subsidizing healthy food to make it affordable for the mass population. Open and safe spaces need to be developed to encourage physical activities among all age groups. Workshops could be run in schools to educate children about healthy food habits and games. Additionally, mobile clinics need to be set up to reach and diagnose early and an informal group to provide counselling to sufferers of NCDs. Also, dedicated and controlled media should be used to teach healthy cooking with a budget to the masses. Fitness clubs could be formed at the local level to promote walking, yoga and similar activities together. The population needs to be educated frequently about age-specific routine medical checkups both at home and at the workplace to know early and treat early. This issue requires the collaboration of government, community and individuals to live a happy and healthy life. Our old age practices of fasting once a week along with several festivals across religions also indicate methods towards a healthy and balanced lifestyle. Another significant step would be increasing health insurance to the masses to confront tough medical situations easily.
Governments can make significant contributions to containing NCDs by increasing t axes on unhealthy packed food and simultaneously subsidizing healthy food to make it affordable for the mass population. Open and safe spaces need to be developed to encourage physical activities among all age groups. Workshops could be run in schools to educate children about healthy food habits and games. Additionally, mobile clinics need to be set up to reach and diagnose early and an informal group to provide counselling to sufferers of NCDs. Also, dedicated and controlled media should be used to teach healthy cooking with a budget to the masses. Fitness clubs could be formed at the local level to promote walking, yoga and similar activities together. The population needs to be educated frequently about age-specific routine medical checkups both at home and at the workplace to know early and treat early. This issue requires the collaboration of government, community and individuals to live a happy and healthy life. Our old age practices of fasting once a week along with several festivals across religions also indicate methods towards a healthy and balanced lifestyle. Another significant step would be increasing health insurance to the masses to confront tough medical situations easily.
REFERENCES
Lifestyle Diseases and Quality of Life Allen, L., Williams, J., Townsend, N., Mikkelsen, B., Roberts, N., Foster, C., & Wickramasinghe, K. (2017). Socioeconomic status and non communicable disease behavioural risk factors in low-income and lower middle-income countries: a systematic review. The Lancet Global Health, 5(3), e277-e289. Balasubramani, K., Paulson, W., Chellappan, S., Ramachandran, R., Behera, S. K., & Balabaskaran Nina, P. (2021). Epidemiology, Hot Spots, and Sociodemographic Risk Factors of Alcohol Consumption in Indian Men and Women: Analysis of National Family Health Survey-4 (2015-16), a Nationally Representative Cross-Sectional Study. Frontiers in public health, 9, 617311. https://doi.org/10.3389/ fpubh.2021.617311 Bobo, J. K., & Husten, C. (2000). Sociocultural i nfluences on smoking and drinking. Alcohol research & health : the journal of the National Institute on Alcohol Abuse and Alcoholism, 24(4), 225–232. Carballo, M. (2009). Communicable diseases. Health and migration in European Union: better health for all in an, 2006, 11-28. Central Bureau of Health Intelligence. (2024). National Health Profile 2023 18th Issue. Directorate General of Health Services Ministry of Health & Family Welfare. Congdon P. (2019). Obesity and Urban Environments. International journal of environmental research and public health, 16(3), 464. https://doi.org/ 10.3390/ijerph16030464 Dutt, B., & Pandey, R. K. (2024). Indigenous Approach to One Health Framework: Integration of Sustainable Solution. Indian Journal of Preventive & Social Medicine, 55(4), 266-274. Fast Food Consumption by Country 2024. (2024-12-14). World Population Review. https://worldpopulationreview.com/ c ountry-rankings/fast-food consumption-by-country Gandhi, M. K. (1948). Key to health. Navajivan Publishing House. Joshi, A. B., & Mahajan, D. P. PREVALENCE AND RISK FACTORS FOR CHRONIC KIDNEY DISEASE (CKD) IN A CROSS SECTIONAL POPULATION STUDY. Mathur, P., & Mascarenhas, L. (2019). Life style Diseases: Keeping Fit for a Better Tomorrow. The Indian journal of medical research, 149(Suppl), S129–S135. https://doi.org/10.4103/0971 5916.251669 Mishra, V. K., Srivastava, S., Muhammad, T., et al. (2022). Relationship between tobacco use, alcohol consumption and non-communicable diseases among women in India: Evidence from National Family Health Survey-2015-16. *BMC Public Health*, *22*, 713. https:// doi.org/https://doi.org/10.1186/ s12889-022-13191-z Patel, A. (2018, July 31). Lifestyle diseases in India. Press Information Bureau, Government of India, Ministry of Health and Family Welfare. https://pib.gov.in/ PressReleasePage.aspx?PRID=1539262 Prasad, D. S., Kabir, Z., Dash, A. K., & Das, B. C. (2012). Prevalence and risk factors for metabolic syndrome in Asian Indians: A community study from urban Eastern India. Journal of cardiovascular disease research, 3(3), 204-211. Rao, K., Goswami, V., & Chandel, S. (2024). Quality of Life and Its Biopsychosocial Determinants: A Study Among the Yadav Community From Delhi, India. Cureus, 16(2). Rai, B., Bramhankar, M. (2021). Tobacco use among Indian states: Key findings from the latest demographic health survey 2019–2020. Tobacco Prevention & Cessation, 7(March), 19. https:// doi.org/10.18332/tpc/132466 Shaikh, R., & Khan, J. (2021). Clustering of l ifestyle risk factors among adult population in India: a cross-sectional analysis from 2005 to 2016. PloS one, 16(1), e0244559. Sharma, M., Gaidhane, A., & Choudhari, S. G. (2024). A Comprehensive Review on Trends and Patterns of Non communicable Disease Risk Factors in India. Cureus, 16(3), e57027. https:// doi.org/10.7759/cureus.57027 Singh, A. K., Maheshwari, A., Sharma, N., & Anand, K. (2006). Lifestyle associated risk factors in adolescents. The Indian Journal of Pediatrics, 73, 901-906. Schraufnagel, D. E., Balmes, J. R., Cowl, C. T., De Matteis, S., Jung, S. H., Mortimer, K., Perez-Padilla, R., Rice, M. B., Riojas Rodriguez, H., Sood, A., Thurston, G. D., To, T., Vanker, A., & Wuebbles, D. J. (2019). Air Pollution and Noncommunicable Diseases: A Review by the Forum of International Respiratory Societies’ Environmental Committee, Part 2: Air Pollution and Organ Systems. Chest, 155(2), 417 426. https://doi.org/10.1016/ j.chest.2018.10.041 Singh, R., Ota, S., Khanduri, S., Rani, S., Bhadula, A., Sharma, R., … & Dhiman, K. S. (2018). Integration of ayush (AYURVEDA and yoga) with national programme for prevention and control of cancer, diabetes, cardiovascular diseases and stroke (NPCDCS): An appraisal of central council for research in ayurvedic sciences research and development initiatives. Journal of Research in Ayurvedic Sciences, 2(1), 27-36. Srivastava, S., & Sureka, R. K. (2024). Efficacy of Ayurveda in the Prevention of Lifestyle Diseases or Non-Communicable Diseases (NCDs). Journal of Ayurveda and Integrated Medical Sciences, 9(8), 122-128. Subramanian, S. V., Corsi, D. J., Subramanyam, M. A., & Davey Smith, G. (2013). Jumping the gun: the problematic discourse on socioeconomic status and cardiovascular health in India. International journal of epidemiology, 42(5), 1410-1426.
Lifestyle Diseases and Quality of Life Allen, L., Williams, J., Townsend, N., Mikkelsen, B., Roberts, N., Foster, C., & Wickramasinghe, K. (2017). Socioeconomic status and non communicable disease behavioural risk factors in low-income and lower middle-income countries: a systematic review. The Lancet Global Health, 5(3), e277-e289. Balasubramani, K., Paulson, W., Chellappan, S., Ramachandran, R., Behera, S. K., & Balabaskaran Nina, P. (2021). Epidemiology, Hot Spots, and Sociodemographic Risk Factors of Alcohol Consumption in Indian Men and Women: Analysis of National Family Health Survey-4 (2015-16), a Nationally Representative Cross-Sectional Study. Frontiers in public health, 9, 617311. https://doi.org/10.3389/ fpubh.2021.617311 Bobo, J. K., & Husten, C. (2000). Sociocultural i nfluences on smoking and drinking. Alcohol research & health : the journal of the National Institute on Alcohol Abuse and Alcoholism, 24(4), 225–232. Carballo, M. (2009). Communicable diseases. Health and migration in European Union: better health for all in an, 2006, 11-28. Central Bureau of Health Intelligence. (2024). National Health Profile 2023 18th Issue. Directorate General of Health Services Ministry of Health & Family Welfare. Congdon P. (2019). Obesity and Urban Environments. International journal of environmental research and public health, 16(3), 464. https://doi.org/ 10.3390/ijerph16030464 Dutt, B., & Pandey, R. K. (2024). Indigenous Approach to One Health Framework: Integration of Sustainable Solution. Indian Journal of Preventive & Social Medicine, 55(4), 266-274. Fast Food Consumption by Country 2024. (2024-12-14). World Population Review. https://worldpopulationreview.com/ c ountry-rankings/fast-food consumption-by-country Gandhi, M. K. (1948). Key to health. Navajivan Publishing House. Joshi, A. B., & Mahajan, D. P. PREVALENCE AND RISK FACTORS FOR CHRONIC KIDNEY DISEASE (CKD) IN A CROSS SECTIONAL POPULATION STUDY. Mathur, P., & Mascarenhas, L. (2019). Life style Diseases: Keeping Fit for a Better Tomorrow. The Indian journal of medical research, 149(Suppl), S129–S135. https://doi.org/10.4103/0971 5916.251669 Mishra, V. K., Srivastava, S., Muhammad, T., et al. (2022). Relationship between tobacco use, alcohol consumption and non-communicable diseases among women in India: Evidence from National Family Health Survey-2015-16. *BMC Public Health*, *22*, 713. https:// doi.org/https://doi.org/10.1186/ s12889-022-13191-z Patel, A. (2018, July 31). Lifestyle diseases in India. Press Information Bureau, Government of India, Ministry of Health and Family Welfare. https://pib.gov.in/ PressReleasePage.aspx?PRID=1539262 Prasad, D. S., Kabir, Z., Dash, A. K., & Das, B. C. (2012). Prevalence and risk factors for metabolic syndrome in Asian Indians: A community study from urban Eastern India. Journal of cardiovascular disease research, 3(3), 204-211. Rao, K., Goswami, V., & Chandel, S. (2024). Quality of Life and Its Biopsychosocial Determinants: A Study Among the Yadav Community From Delhi, India. Cureus, 16(2). Rai, B., Bramhankar, M. (2021). Tobacco use among Indian states: Key findings from the latest demographic health survey 2019–2020. Tobacco Prevention & Cessation, 7(March), 19. https:// doi.org/10.18332/tpc/132466 Shaikh, R., & Khan, J. (2021). Clustering of l ifestyle risk factors among adult population in India: a cross-sectional analysis from 2005 to 2016. PloS one, 16(1), e0244559. Sharma, M., Gaidhane, A., & Choudhari, S. G. (2024). A Comprehensive Review on Trends and Patterns of Non communicable Disease Risk Factors in India. Cureus, 16(3), e57027. https:// doi.org/10.7759/cureus.57027 Singh, A. K., Maheshwari, A., Sharma, N., & Anand, K. (2006). Lifestyle associated risk factors in adolescents. The Indian Journal of Pediatrics, 73, 901-906. Schraufnagel, D. E., Balmes, J. R., Cowl, C. T., De Matteis, S., Jung, S. H., Mortimer, K., Perez-Padilla, R., Rice, M. B., Riojas Rodriguez, H., Sood, A., Thurston, G. D., To, T., Vanker, A., & Wuebbles, D. J. (2019). Air Pollution and Noncommunicable Diseases: A Review by the Forum of International Respiratory Societies’ Environmental Committee, Part 2: Air Pollution and Organ Systems. Chest, 155(2), 417 426. https://doi.org/10.1016/ j.chest.2018.10.041 Singh, R., Ota, S., Khanduri, S., Rani, S., Bhadula, A., Sharma, R., … & Dhiman, K. S. (2018). Integration of ayush (AYURVEDA and yoga) with national programme for prevention and control of cancer, diabetes, cardiovascular diseases and stroke (NPCDCS): An appraisal of central council for research in ayurvedic sciences research and development initiatives. Journal of Research in Ayurvedic Sciences, 2(1), 27-36. Srivastava, S., & Sureka, R. K. (2024). Efficacy of Ayurveda in the Prevention of Lifestyle Diseases or Non-Communicable Diseases (NCDs). Journal of Ayurveda and Integrated Medical Sciences, 9(8), 122-128. Subramanian, S. V., Corsi, D. J., Subramanyam, M. A., & Davey Smith, G. (2013). Jumping the gun: the problematic discourse on socioeconomic status and cardiovascular health in India. International journal of epidemiology, 42(5), 1410-1426.
Conflict of interest: None
Role of funding source: None
