A generic phrase used to describe unpleasant
feelings or emotions that affect a person’s
level of functioning is psychological distress.
Well-being status is experienced as health,
happiness, and prosperity. It includes having
good mental health, high life satisfaction, a
sense of meaning and purpose, and the ability
to manage stress. Various reasons have led
to several changes in our day-to-day activities
due to social distancing, lockdown, and other
health hygiene practices, which are
continuously influencing psychological distress
and creating obstacles to well-being.
The primary objective of this study is to
measure the psychological distress and public
health measures associ ated with i t s
containment, and to provide mental health
intervention policies to cope with thi s
challenge. The present study has taken up for
study the two variables: psychological distress and well-being. The relationship between the
two variables holds significance, especially in
the population of adults. Young adults are in
a stage where they might be suffering from
unemployment, fear of job loss and peer
group, academic changes, relationship
conflicts, economic crisis, etc. So, it is also
quite natural that they might go through some
mental health crises and lack of well-being.
Consequently, an effort has been undertaken
to evaluate the level of psychological distress
and well-being of adults. This will help to
formulate appropriate intervention measures
to reduce the problem.
Well-Being: A comprehensive state of wellbeing, not only the absence of disease or
infirmity, which includes one’s physical,
mental, and social aspects (WHO, 1948).
Health is framed as a positive objective since
“wellbeing” denotes a positive rather than
neutral condition.
Psychological Distress: Psychological
distress is a state of emotional suffering
associated with depression, anxiety, and
stress that is difficult to cope with in daily life.
A Sheet of Demographic Information: A
demographic information sheet will be used
to collect various demographic information
about the sample, including age, gender,
education, qualification, and marital status.
The Depression, Anxiety, and Stress Scale
(DASS) (Lovibond& Lovibond et al., 2017):
World Health Organization-Five Well-Being
Index (WHO Regional Office, Europe, 1998)
WHO-5 is the 5-item Well-Being Index, the
4 2
Psychological Distress and Well-Being: A Cross-sectional Study of Adults in Asansol
Indian Journal of Health Social Work. 4(1) January-June, 2022
most widely used questionnaire for assessing
subjective psychological well-being. It consists
of five statements, which respondents’ rate
according to the scale in relation to the past
two weeks.
A more or less equal proportion of male and
female respondents was found in the study
sample. Only 13% of the adults were married,
and the remaining 87% were unmarried. The
educational status of all the respondents
ranges from 12th grade to M. A maximum of
three of them can be third-year grad or firstyear master’s students. If we see the age
pattern of the adult respondents, the average
age of the adult respondents is 25, the
minimum age is 18, and the maximum age of
the adult respondents is 61.
Age is strongly associated and varies with the
psychological distress and wellbeing of the
adult respondents. With an increase in age,
there is a variation in psychological distress
and wellbeing status has been found among
adults (Zautra AJ et. al. 2005). Depression
status and stress were also significantly
associated and varied among the respondents
between different age groups (Roberts RE et
al. 2010). The anxiety level does not show
significant variation among the adult
respondents, although different studies have
found that significant variation among the
adult respondents exists (Lahey et al. 2005).
Age and education have a positive
relationship. As people age, their educational
status seems to improve among the adult
respondents. There is a negative relationship
between increasing age and the level of
depression, anxiety, and stress among adult
respondents. As a result, with increasing age,
there is a lower chance of experiencing
depression, anxiety, and stress among adult
respondents (Keyes et al. 2005). The WHO’s
wellbeing status seems to be improving with increasing age. That shows the positive
relationship between age and wellbeing status
among adult respondents (Andrews G et al.
2011). When we examine the relationship
between educational attainment and
psychological stress and well-being, we find
that as educational attainment increases, the
prevalence of depression, anxiety, and stress
decreases, as all variables have a negative
relationship with educational attainment
(Smith TB et al. 2009). In adults, the WHO
wellbeing status has a positive relationship
with education level (Herrman H et al. 2001).
If we see the co-relation between stress and
anxiety with depression, it shows a strong
positive relationship. That means, with
increasing stress and anxiety, the prevalence
of depression also increases (Freidli L et al.
2009). There is a negative correlation
between WHO we ll-being status and
depression among the adult respondents. As
a result, highly depressed people have a lower
quality of life (Diener E et al.2003). Anxiety
and depression have a significant positive
association among the adult respondents.
That means, with increasing stress, the level
of anxiety also increases (Diener E et al.1985).
Finally, there is a negative correlation between
stress and the WHO well-being status of adult
respondents. As a result, highly stressed
people have less well-being in life (Deci EL et
al. 2008).
The result is that there is no significant age
variation among the male and female adult
respondents on the basis of age pattern.
There is no gender difference on the basis of
educational status among male and female
respondents. If we look at the depression
status, there is a significant gender variation
that exists among the male and female
respondents. On the basis of anxiety level,
there is a slight variation between male and
female respondents; females have more
anxiety than male adult respondents (Dear K
et al. 2002). Stress levels differ significantly between male and female respondents, with
females being more stressed than male adult
respondents (Cohen S et al. 2007). Gender
differences also exist on the basis of the WHO
well-being scale among male and female
respondents. Male respondents have a higher
well-being status than female adult
respondents (Boehm JK et al. 2011).
This research pap er deals with the
psychological distress and well-being among
adults in Asansol. From the study, it is clear
that age, education, and marital status show
significant correlation and association with
psychological distress and wellbeing among
adults. There is a certain level of gender
differentiation on the basis of depression,
anxiety, and stress among male and female
adults. Women are more likely to experience
despair, anxiety and stress than male adults.
There is not so much government planning
and policies on mental health issues among
adults. Our study emphasises the need to pay
attention to the effects of such lockdowns on
the mental wellbeing of adults.
Boehm, J. K, Peterson, C., Kivimaki, M.,
Kubzansky, L. (2011). A prospective
study of positive psychological wellbeing and coronary heart
disease, Health Psychology, 30: 259–
267
Cohen, S., & Lemay, E. P. (2007). Why would
social networks be linked to affect and
health prac tices? Health
Psychology, 26: 410–417.
Dear, K., Henderson, S., & Corten, A. (2002).
Well-being in Australia: Findings from
the national survey of mental health
and well-being. Social Psychiatry and
Psychiatric Epidemiology, 37: 503–
509.
Deci, E. L., & Ryan RM. (2008). Hedonia,
4 5
Psychological Distress and Well-Being: A Cross-sectional Study of Adults in Asansol
Indian Journal of Health Social Work. 4(1) January-June, 2022
eudaimonia, and well-being: An
introduction. Journal of Happiness
Studies, 9: 1–11.
Diener, E., Emmons, R. A., Larson, R. J., &
Griffin, S. (1985). The satisfaction with
life scale. Journal of Personality
Assessment, 49: 71–75
Diener, E., Scollon, C. K. N., Oishi, S., Dzokoto,
V., & Suh, E. M. (2000). Positivity and
the construction of life satisfaction
judgements: Global happiness is not
the sum of its parts. Journal of
Happiness Studies, 1: 159–176.
Diener, E., Oishi, S., & Lucas, R. E. (2003).
Personality, culture, and subjective
wellbeing: Emotional and cognitive
evaluations of life. Annual Review of
Psychology, 54: 403–425.
Foresight Mental Capital and Wellbeing
Project. (2008). Mental Capital and
Wellbeing: Making the most of
ourselves in the 21st century –
Executive Summary. Government
Office for Science, London.
Freidli, L. (2009). Mental health, resilience and
inequal ities . Wo rld Health
Organisation Europe, Copenhagen
Herrman, H. (2001). The need for mental
health promotion. Australian and New
Zealand Journal of
Psychiatry, 35: 709–715.
Holt-Lunstad, J., Smith, T. B., & Layton, J. B.
(2010). Social relationships and
mortality risk: A meta-analytic
review. PLoS Medicine, 7.
Huppert, F. A. (2009). Psychological wellbeing: Evidence regarding its causes
and consequences. Applied
Psychology: Health and Well
Being, 1: 137–164.
Campion, J., Javed, A., Sartorius, N.,
& Marmot, M. (2020). Addressing the
public mental health challenge of
COVID-19, Lancet Psychiatry, 7,
pp. 657-65.
Brooks, S. K., Webster, R. K., Smith, L. E.,
Woodland, L., Wessely, S., Greenberg,
N., & Rubin, G. J. (2020). The
psychological impact of quarantine and
how to reduce it: Rapid review of the
evidence, Lancet, 395, pp. 14-20.
Conflict of interest: None
Role of funding source: None

 On the basis of gender, a more or less equal proportion of male (51%) and female (49%) respondents were found in the study sample. If we look at the marital status of the respondents, then only 13% of the adults
On the basis of gender, a more or less equal proportion of male (51%) and female (49%) respondents were found in the study sample. If we look at the marital status of the respondents, then only 13% of the adults From the result of the independent t test, we can say that age is strongly associated and varied with psychological distress and wellbeing of the adult respondents. The adult respondents’ educational status does not have a significant association or variation with psychological distress and wellbeing. The respondents’ depression status was also significantly associated and varied among the respondents. Anxiety levels do not show significant variation among the adult respondents. Stress levels also showed significant variation and association among
From the result of the independent t test, we can say that age is strongly associated and varied with psychological distress and wellbeing of the adult respondents. The adult respondents’ educational status does not have a significant association or variation with psychological distress and wellbeing. The respondents’ depression status was also significantly associated and varied among the respondents. Anxiety levels do not show significant variation among the adult respondents. Stress levels also showed significant variation and association among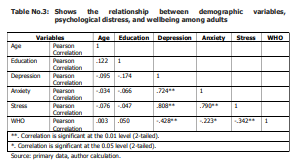 From the Pearson correlation table, we can say that age and education have a positive relationship (.122). With increasing age, educational status seems to improve among the adult respondents. There is a negative relationship between increasing age and the level of depression (-.095), anxiety (-.034), and stress (-.076) among adult respondents, implying that with increasing age comes a lower risk of depression, anxiety, and stress. The WHO wellbeing status (.003) seems to be improving with increasing age. That shows the positive relationship between age and wellbeing status for adult respondents. If we
try to analyse the co-relation between educational status and psychological stress and well-being, it is found that with increasing educational status there is a lower prevalence of depression (-.174), anxiety (-.066) and stress (-.067) as all the variables have a
negative relationship with educational level.
The WHO wellbeing status (0.50) has a
positive relationship with the educational level
among adults. If we see the correlation
between stress (.808) and anxiety (.724) with
depression, it shows a strong positive
relationship. That means with increasing
stress and anxiety, the prevalence of
depression also increases. There is a negative
correlation between WHO well-being status
(-0.424) and depression among the adult
respondents. As a result, highly depressed
people have less well-being in life. There is a
strong positive co-relationship between
anxiety and stress (.790) among the adult
respondents. That means, with increasing
stress, the level of anxiety also increases.
Finally, there is a negative correlation between
stress and the WHO well-being status (-
0.3244) of adult respondents. As a result,
highly stressed people have less well-being
in life.
From the Pearson correlation table, we can say that age and education have a positive relationship (.122). With increasing age, educational status seems to improve among the adult respondents. There is a negative relationship between increasing age and the level of depression (-.095), anxiety (-.034), and stress (-.076) among adult respondents, implying that with increasing age comes a lower risk of depression, anxiety, and stress. The WHO wellbeing status (.003) seems to be improving with increasing age. That shows the positive relationship between age and wellbeing status for adult respondents. If we
try to analyse the co-relation between educational status and psychological stress and well-being, it is found that with increasing educational status there is a lower prevalence of depression (-.174), anxiety (-.066) and stress (-.067) as all the variables have a
negative relationship with educational level.
The WHO wellbeing status (0.50) has a
positive relationship with the educational level
among adults. If we see the correlation
between stress (.808) and anxiety (.724) with
depression, it shows a strong positive
relationship. That means with increasing
stress and anxiety, the prevalence of
depression also increases. There is a negative
correlation between WHO well-being status
(-0.424) and depression among the adult
respondents. As a result, highly depressed
people have less well-being in life. There is a
strong positive co-relationship between
anxiety and stress (.790) among the adult
respondents. That means, with increasing
stress, the level of anxiety also increases.
Finally, there is a negative correlation between
stress and the WHO well-being status (-
0.3244) of adult respondents. As a result,
highly stressed people have less well-being
in life. 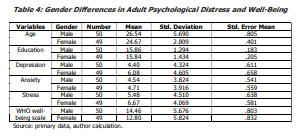 From the statistical table, we can say that there is no significant age variation exists among the male (mean = 26) and female (mean = 25) adult respondents on the basis of age pattern. There is no gender difference on the basis of educational status among male (mean = 16) and female (mean = 16) respondents. If we look at the depression status, there is a significant gender variation that exists among the male (mean = 4.4) and female (mean = 6.1) respondents. On the basis of anxiety level, there is a slight variation between male (mean = 4.5) and female (mean = 4.7) respondents. The stress level shows a significant level of gender differences among male (mean = 5.4) and female (mean = 6.7) respondents. Gender differences also exist on the basis of the WHO well-being scale among male (mean = 4.7) and female (mean = 4.7) respondents.
From the statistical table, we can say that there is no significant age variation exists among the male (mean = 26) and female (mean = 25) adult respondents on the basis of age pattern. There is no gender difference on the basis of educational status among male (mean = 16) and female (mean = 16) respondents. If we look at the depression status, there is a significant gender variation that exists among the male (mean = 4.4) and female (mean = 6.1) respondents. On the basis of anxiety level, there is a slight variation between male (mean = 4.5) and female (mean = 4.7) respondents. The stress level shows a significant level of gender differences among male (mean = 5.4) and female (mean = 6.7) respondents. Gender differences also exist on the basis of the WHO well-being scale among male (mean = 4.7) and female (mean = 4.7) respondents.