
Indian Journal of Health Social Work
(UGC CARE List Journal)
INTERACTION PATTERNS IN THE FAMILIES OF INDIVIDUAL WITH CANNABIS DEPENDENCE
Nirmala Kumari Ahirwar1 & Manisha Kiran2
1Ph. D Scholar (PSW), Department of Psychiatric Social Work, Ranchi Institute of Neuro-Psychiatric and Allied Science, Jharkhand India. 2Associate Professor & Head, Department of Psychiatric Social Work, Ranchi Institute of Neuro-Psychiatric and Allied Science, Jharkhand India Correspondence: Nirmala Kumari Ahirwar, e-mail: nirmalakumariahirwar@gmail.com
ABSTRACT
Background:Cannabis dependency is often due to prolonged and increasing use of the drug. Increasing the strength of the cannabis taken and an increasing use of more effective methods of delivery often increase the progression of cannabis dependency. Interaction pattern in a family has been found critical tasks in keeping family development, system and well-being as well as maintaining its integrity.
Aim:
This study was planned to see the family interaction pattern of individuals with cannabis dependence in Indian setting.
Method:
The study was a cross sectional, hospital based and the samples were selected through purposive sampling technique. This study was included 30 individuals (patients diagnosed with cannabis dependence as per ICD -10) and 30 individuals from family of normal controls (i.e., a family without any cannabis dependence member). Age, education and family income matched with either group.GHQ-12 & Family Interaction Pattern Scale were applied on all the selected individuals in the study.
Results and Conclusion:
Dysfucntional interaction was found in the domains of “reinforcement”, “social support”, “roles”, “communication”, & “total FIPS” in the families of individual with cannabis dependence as compared to families of normal controls.
Keyword: Family interaction pattern, cannabis dependence, indian families.
INTRODUCTION
Family interaction patterns were defined as those various social psychological transactions occurring in the family as a system, to evolve process for decision making, emotional expressions and personal view, assigning tasks and social status, enabling the family member to contribute for the growth of the family by generating morphogenesis at emotional, intellectual and social levels through the manipulation of internal and external social milieu of the family as a whole. According to the evolutionary point of view every family has patterns of leadership, communication, role, cohesiveness, and social support system which were defined as follows. Leadership: A family member engaged in decision making through consensus for the growth of the family as a system is the leader of the family. Communication: Processes through which the family members convey their feelings, emotions and personal views. Roles: Socioculturally prescribed and ascribed tasks to be performed by different family members according to their age and sex . Reinforcement: Processes adopted by the family to enable the members to imbibe socially approved behavior. Cohesiveness: Process adopted by the family for a firm degree of mutual trust and interpersonal commitment. Social support: Social support system refers to manipulation of internal and external social milieu of the family for its existence and growth (Bhatti et al., 1986). Family interactions of substance use, and the potential effect of cannabis on those interactions, has been a consistent concern in both the clinical and research literature for more than 20 years. Some authors like Jacob et al (1981) suggests that cannabis and other substance families differ from without cannabis families in affective expression, as reflected in lower rates of positive affect and higher rates of negative affect. These differences seem to characterize parent child interactions. However some studies also characterize interactions between the male cannabis and his spouse (Jacob & Krahn, 1988). Thus it was evident that cannabis consumption not only causes disturbance in interactional pattern between parent’s children but also between marital couples. In those studies family distress and marital distresses were equally emphasized. Although most studies in the cannabis smoke and marriage literature have emphasized the personality traits and characteristics of spouses, behavioral systems theories of the past decade have directed increasing attention toward interaction variables that might elicit and maintain cannabis abuse. The most elaborate of these models, proposed by Steinglass (1981), has incorporated the provocative hypothesis that cannabis can serve adaptive functions in some families and as a result be reinforced and perpetuated through change in family processes. Most relevant to this, is a cross sectional finding by Jacob et al (1978) that revealed a negative relation between the husband’s substance consumption and the wife’s psychiatric symptomatology and a positive relation between the husband’s alcohol consumption and the wife’s marital satisfaction, findings that emerged only with steady drinkers and not with binge drinkers. In a study by Frankenstein et al (1985) found that cannabis increased positive interactions, whereas two studies by Jacob and his colleagues found that substance use (i.e. alcohol & cannabis) increased negative interactions of alcoholics and their spouses (Jacob et al, 1981; Jacob & Krahn, 1988) indicating that alcohol does exert an impact on marital interactions of alcoholics, although the direction of such effects has not been entirely consistent across studies. Various cross-study differences in methodology could be related to these discrepant findings, including differences in experimental task, dose level, administration format, and the presence or absence of comparison groups (Chakravarthy, 1990).
AIM
The present study was carried out to examine the family interaction patterns in Indian families with individual of cannabis dependence.
MATERIALS AND METHODS
Design
This was a cross-sectional study and carried out among families of patients who came at Ranchi Institute of Neuro-Psychiatry and allied science (RINPAS), a state government- owned psychiatric hospital situated in the Ranchi district of Jharkhand State in India.The ‘purposive sampling method’ was used.
Participants
The sample consisted of 30 families of male patients diagnosed with cannabis dependence syndrome (CDS) using the criteria laid out in the ICD-10 (WHO, 1993) and 30 families of appropriately matched males (control group) with no history of cannabis dependence, who scored less than 3 on the GHQ-12. Inclusion and exclusion criteria were as follows. The experimental group was made up of families diagnosed as having ‘Mental and behavioural disorders due to use of cannabis’ from the RINPAS according to the ICD-1 0 Classification of Mental and Behavioural Disorders – Diagnostic Criteria for Research (ICD-10 DCR). Those who had been married for 2 or more years, scored less than 3 in the General Health Questionnaire–12 (GHQ-12), were free from major physical illnesses, and who gave their informed consent to participation in the study were included. The families of control group were selected after matching their ages, educational and income levels with the experimental group and scored less than 3 in the GHQ-12, no history of major physical illnesses, and gave their informed consent to participation in the study.
TABLE 1: Comparison of Socio-demographic characteristics of families with and without Cannabis Dependent.

TABLE 2: Comparison of Socio-demographic characteristics of families with and without
Cannabis Dependent.
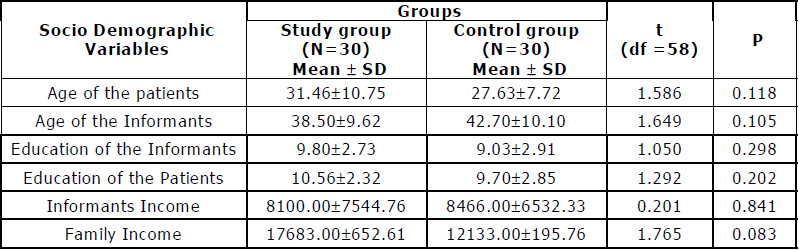
TABLE 3: Comparison of families with and without Cannabis Dependent on domain of
Family Interaction Pattern Scale.

The present study was conducted on the Out Patient Department of the Ranchi Institute of Neuro Psychiatry & Allied Sciences (RINPAS), Kanke, Ranchi. It was based on purposive sampling technique. This was a comparative study and 30 families from the patients diagnosed with cannabis dependence and 30 of families from normal controls (i.e., a family without any cannabis dependence member). This study was planned to assess the interaction patterns in the families of patients with cannabis dependence and families of normal controls.
The result of the present indicated that there was significant difference between the families with and without cannabis dependents in various areas of family interaction pattern scale. We found that families with cannabis dependent s perceived dysfunctional interaction pattern as compared to families without cannabis dependents. The mean of present study was found significantly higher in the various domains of t he family interaction pattern scale i.e. “reinforcement”, “social support”, “role”, “communication” & “Total FIPS” in the families of cannabis dependents as compared to families without cannabis dependents. Present study finding implicate significant dysfunctions in interaction patterns in families with cannabis dependents. The dysfunction is widespread and encompasses are as such as reinforcement , social support, role, communication, and so forth. Impaired interaction pattern in families of cannabis dependents, manifesting in the form of poor family support and communication marred with negative connotations has been highlighted by various previous researchers with population of alcohol and substance use (Suman & Nagalakkshmi, 1995; Jacob & Seilhamer, 1989; Christine & Victor 1993; Akhito et al., 2003) and, therefore, the findings of this study is in consonance. Impaired interaction pattern can have serious implications as far as substance is concerned. In fact, it can have implication from both cause as well as effect perspectives. For example, on the one hand, a person can become vulnerable for cannabis consumption due to persistent nagging as a result of negative communication and, on the other; hi s cannabis / substance consumption behaviour can force the family members to make negative comments on him. It applies to other sub-domains of interaction pattern as well. For example, a person can have deficient role functioning due to his substance consumption behaviour while poor role assignment can leave a person despondent and make him vulnerable for cannabis and substance use. A strong parent–child relationship is an important protective factor in preventing substance abuse in the families (Davis & Spillman, 2011). A positive and protective relationship is determined by the degree of parental intimacy, expression of excitement and pride for success and skills of the child, and expression of intimacy and love (Amato, 1990). Studies have demonstrated that qualified interaction between parents and the child, consistent and effective discipline methods, and a positive parenting model reduce the risk to consume substance use disorders (Ogel et al., 2004).
CONCLUSION
Finding of the present study concludes that Cannabis can have a negative effect on various areas of the family interaction pattern i.e “reinforcement”, “social support”, “role”, “communication” So, it is know that individual with cannabis dependents has significant impact on interaction patterns and it has become significant predictors and tends to appear among the families who have spent some years in their caring and service of the individuals with cannabis users. Present study has some limitations i.e. the sample size is small and is cross-sectional . The other variables like that treatment adherence and duration of taking cannabis have not been included. Cultural factors are also important in this issue but the effects of race and ethnicity have no t been ta ken into consideration in this study.
REFERENCES
Akihito, H., Kim, T., & Koichi, N.(2003). Positive and Negative Effects of Social Support on the Relationship between Work Stress and Alcohol Consumption. Journal of Studies on Alcohol, 64, 874-883.
Amato, P.(1986). Dimensions of the family environment as perceived by children: A mul t i dimens ional s c al i ng s tudy. Journal of Mar r iage and Family, 19, 52, 613–620.
Bhatti, S.R., Cuba, K.D.K., & Benedicta, L.A. (1986). Val idation of Fami ly Interaction Pattern Scale. Indian Journal of Psychiatry, 28, 211-216.
Chakravarthy (1990). Community workers estimate of drinking and alcoholrelated problems in rural areas. Indian Journal of Ps ychologi cal Medicine, 13, 49-56.
Christine, M.O., & Victor, M.H.( 1993). The influence of perceived social support on the relationship between family history of alcoholism and drinking behaviors. Addiction, 88, 1651-1658.
Davis, S.J., & Spillman, S.(2001). Reasons for drug abstention: A study of drug use and resilience. Journal of Psychoactive Drugs, 43, 14–19.
Frankenstein, W., Hay, W.M., & Nathan, P.E.(1985). Effects of intoxication on alcoholics’ marital communication and problem solving. Journal of Studies on Alcohol , 46, 1-6.
Goldberg, D.P., & William, P.(1978). A user guide to General Health Questionnaire. Windsor, NFER-Nelson,.
Jacab, T., Richey, D., Evitkovic, J.F., & Blane, H.T. (1981). Communications styles of alcoholic and nonalcoholic families when drinking and not drinking. Journal of Studies on Alcohol, 42, 466-482.
Jacob, T., & Sei lhamer, R.A. (1989) . Alcoholism and family interaction. Recent Developments in Alcoholism, 7, 129-145.
Jacob, T., Favorini, A., Meisel, S., & Anderson, C. (1978). The spouse, Children and family interactions of the alcoholic: Substantive findings and methodological issues. Journal of Studies on Alcohol , 39, 1231-1251.
Jacob, T., & Krahn, G. (1988) . Mar i tal interaction of alcohol ic couples: Comparison with depressed and nondi s t re s se d coupl es . Jo ur na l of Consulting and Clinical Psychology , 56,73-79.
Ogel , K., Taner, S., & Eke, C.Y.(2004). Evaluating the effectiveness of the teacher and parent education program in addiction prevention. Anatolian Journal of Psychiatry, 5, 213–221.
Steinglass, P.(1981). The impact of alcoholism on the family: Relationship between degree of alcoholism and psychiatric symptomatology. Journal of Studies on Alcohol, 42, 288-303.
Suman, L.N., & Nagalakshmi, S.V.(1995). Family interaction patterns in alcoholic families. NIMHANS Journal , 13, 47- 52.
World Health Organisation, (1993).The ICD- 10 class i f icat ion of mental and behavioural disorders –diagnostic criteria for research. WHO, Geneva.
Conflict of interest: None
Role of funding source: None
It’s a matter of great pride for me that All India Association of Medical Social Work Professionals is launching first issue of “Indian Journal of Health Social Work” on the auspicious occasion of 6th Annual National Conference of AIAMSWP, 2019.
I visited several sites but the audio quality for audio songs existing at this web page is truly marvelous.
It’s amazing designed for me to have a site, which is good in favor of my experience. thanks admin
Hi there every one, here every one is sharing these know-how, thus it’s nice to read this blog, and I used to pay a quick visit this weblog all the time.
One more main part of addiction treatment is behavior modifications.
I am really impressed with your writing abilities as well as with the format to your weblog. Is that this a paid theme or did you modify it yourself? Either way stay up the excellent quality writing, it is uncommon to see a nice blog like this one these days..
Does your site have a contact page? I’m having a tough time locating it but, I’d like to shoot you an e-mail. I’ve got some ideas for your blog you might be interested in hearing. Either way, great website and I look forward to seeing it grow over time.
Why people still make use of to read news papers when in this technological world the whole thing is presented on net?
I was curious if you ever considered changing the layout of your website? Its very well written; I love what youve got to say. But maybe you could a little more in the way of content so people could connect with it better. Youve got an awful lot of text for only having 1 or two images. Maybe you could space it out better?
Everything is very open with a clear explanation of the challenges.
It was really informative. Your site is useful.
Many thanks for sharing! http://worldmissionship.com/words/1575166
Every weekend i used to pay a quick visit this website, because i want enjoyment, since this this site conations really nice funny stuff too.